|
HPI: 83 year old caucasian male with a past medical history of atrial fibrillation, COPD, HTN, metastatic prostate cancer, presented to ED after a ground level fall, found to have altered mental status, cerebral edema with midline shift, no intracranial bleeding. 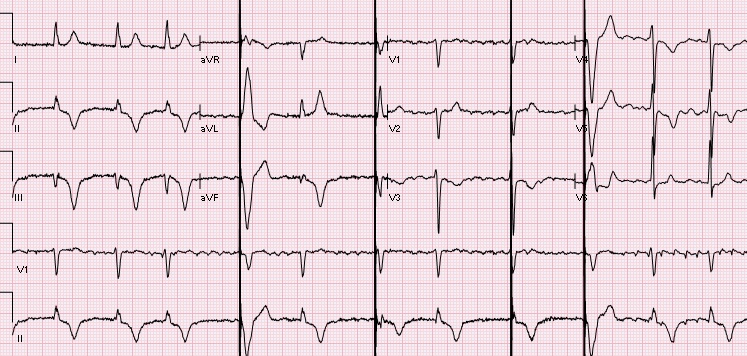 EKG: Auto read: Demand pacemaker; interpretation is based on intrinsic rhythm. Atrial fibrillation with premature ventricular or aberrantly conducted complexes. Cannot rule out Inferior infarct, age undetermined. ST & T wave abnormality, consider anterolateral ischemia or digitalis effect. Abnormal ECG. No previous ECGs available.
Let's discuss this EKG. Ventricular rate is in the 60-70s, rhythm is definitely not sinus, as there are not a p wave before every QRS. The P waves, in fact, are absent. Axis is normal (upgoing QRS in I & aVF). The QRS is upgoing in Lead I suggestive of left ventricular pacing. QRS is not wide, QT is not prolonged. There are deep negative T waves in II, III, aVF, V4, and V5. There is normal R wave progression. Deep T waves in this EKG are a result of a phenomenon known as Cardiac Memory. These are NON-ISCHEMIC T wave inversions that are a result of repolarization abnormalities in the setting of intermittently wide QRS. So what causes these non-ischemic t-wave inversions? Well, first the QRS must become intermittently wide, as is seen in demand pacing (such as in the patient in this case), WPW, prolonged VT, or intermittent LBBB. Then, as the QRS becomes narrow again, the T waves become negative in the leads where QRS was wide. There is a lag in resolution of the repolarization abnormality, which is likely channel related (but poorly understood). The persistence of T wave inversion depends on how frequently the QRS is wide, or in this case, how frequently the heart is LV paced. Basically the T waves are slow to normalize after an episode of widened QRS. There is a broad differential diagnosis for T wave inversion, including subendocardial ischemia, acute CNS bleeds, acute adrenergic stress, PE, metabolic abnormalities, and drug effects. Because of the broad differential, new diffuse T wave inversion should always focus on the "worst first", and in general cardiac memory is a diagnosis of exclusion. Recognizing this characteristic post-pacing T-wave morphology can be a valuable piece of information in your clinical decision making. Ischemia workup is not indicated based on the EKG alone. This transient EKG finding, in conjunction with negative serum cardiac enzymes, absence of chest pain/cardiac complaints, makes cardiac memory the most likely cause of the EKG abnormality. Don't fear the deep inverted T waves in demand pacing! References: Littman, L., Fermant, A. Large T-Wave Inversion in a Patient With a Pacemaker. Arch Intern Med. 2011 Aug 8;171(15):1314-16.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
