|
HPI: A previously healthy, incarcerated, 43 year old Asian American male presented to the ED after a syncopal episode with subsequent VF arrest. The patient is successfully defibrillated. After ROSC the following EKG is obtained: 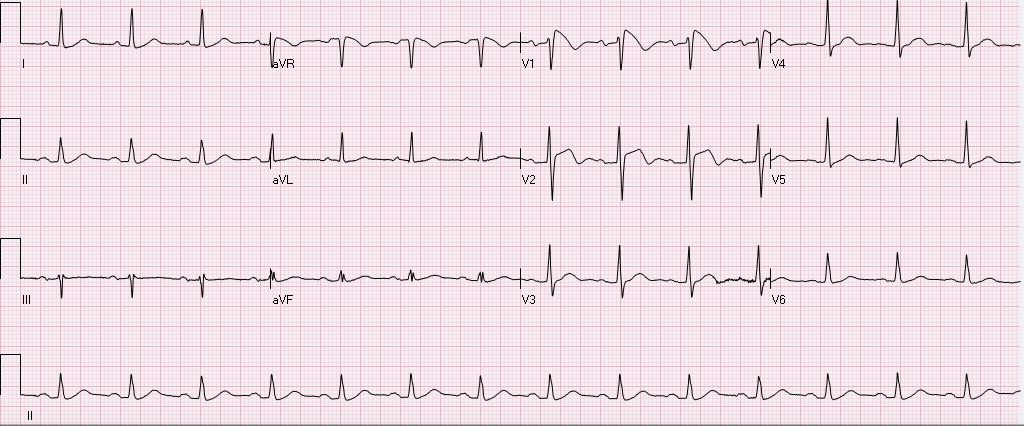 Normal rate, regular rhythm, sinus P waves in from of QRS. normal PR, normal QRS width, axis, amplitude, progression. ST elevation in V1, V2, inverted T waves in V2, normal QTc.
After obtaining this EKG the patient was rushed to the cath lab, no obstructive coronary lesions were identified. What is the diagnosis, and what is the treatment? Is this finding always pathological? The diagnosis is Brugada syndrome. - syndrome is a constellation of Brugada pattern EKG + CLINICAL SYMPTOMS Brugada Pattern EKG: -RBBB pattern in V1 (rSR', terminal positive QRS complex) -high take off, upward convex, ST elevation in V1 and V2 -inverted T waves in V1 and V2 Clinical Symptoms: syncope, +/- palpitations, unexplained VF/arrest, family history of sudden death. Brugada Syndrome: -due to poorly understood sodium chanellopathy. There is NO UNDERLYING STRUCTURAL HEART DISEASE. -except for V1-V2, the EKG is usually normal. -Brugada pattern on EKG can be transient, and can be unmasked by physical stressors, medications, metabolic derangements, and ischemia. Treatment: ICD is indicated for patients with Brugada syndrome. Brugada Pattern EKG is NOT ALWAYS pathalogical. -Brugada pattern EKG can be a normal variant, especially in a patient without risk factors, symptoms, and the pattern is an incidental finding during a non-cardiac workup. -Brugada pattern can also be seen in severe hyperkalemia, sodium-channel blocker toxicity, propofol infusion syndrome, right ventricular pathology or injury. Patients who are incidentally found to have Brugada pattern EKG without cardiac symptoms are at low risk for sudden cardiac death. These patients should be educated on finding, referred to cardiologist, and given careful follow up precautions if they develop syncope, palpitations, chest pain, or other cardiac symptoms. A careful family history to elucidate family members with sudden cardiac death is warranted. There is some risk if the patient has Brugada EKG pattern without symptoms, but does have a family member who experienced sudden cardiac death. These patients should be referred to a cardiologist, and may undergo provocative testing to induce VT/VF, although this is controversial. References: 1. Littmann, L. Monroe, MH., Kerns, WP., Svenson, RH., Gallagher, JJ. Brugada syndrome and "Brugada sign": clinical spectrum with a guide for the clinician. Am Heart J. 2003 May;145(5):768-78. 2. http://lifeinthefastlane.com/ecg-library/brugada-syndrome/
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
