|
A 56 year old female with a history of asthma, hypothyroidism, tobacco use, chronic opioid use was found down at home, found to have subarachnoid hemorrhage, left temporal hematoma with bilateral supraclinoid aneurysms on CTA, s/p embolization. Hospitalization has been complicated by vasospasm, fevers, long QT, and stress induced cardiomyopathy. On hospital day 11 the following EKG was obtained to assess the patient's long QT noted on previous EKGs (500, 516, 620). 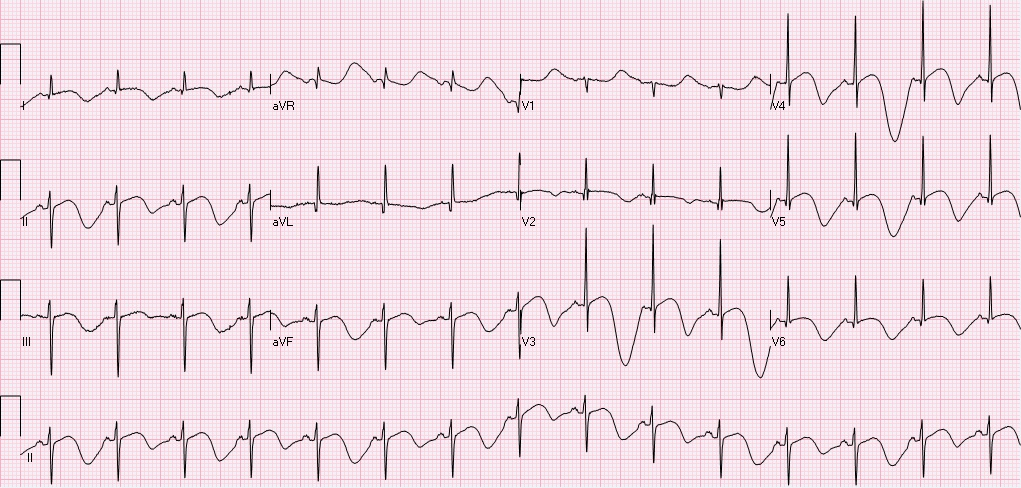 Rate 89, sinus rhythm with sinus p waves, left axis deviation, normal PR, QRS intervals, prolonged QTc 732. T-wave inversions in I, II, III, aVF, V2-V6. In fact, if you pay attention to the T-wave morphology you will notice polymorphic deep t-waves, alternating in depth and morphology. There are two interesting points from this EKG: 1) T-QT pattern, and 2) T wave alternans. T-QT pattern:
T wave alternans:
Approximately 2 hours after the above EKG, the following rhythm strip was noted on telemetry.  Here you see a PVC followed by a compensatory pause, followed by polymorphic VT. Pauses are frequent triggers of Torsades. The patient went on to experience several sustained, and non-sustained runs of polymorphic VT overnight. She received aggressive Mg & K repletion, defibrillator pads were placed, but patient remained hemodynamically stable and did not require defibrillation or overdrive pacing. QT decreased and VT resolved.
Teaching points:
References: Warraich H, Buxton A, Kociol R. Macroscopic T-wave alternans in a patient with takotsubo cardiomyopathy and QT prolongations. Heart Rhythm. 2014 Oct;11(10):1848-9. Sommargren C, Drew B. Preventing torsades de pointes by careful cardiac monitoring in hospital settings. AACN Adv Crit Care. 2007 Jul-Sep;18(3):285-93
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
