|
HPI: 57 y/o woman with remote hx of CABG/PCI presents with 2 hrs of 6-10/10 substernal chest tightness and SOB. No recent cardiac events/complaints. Initial troponin is 1.48. 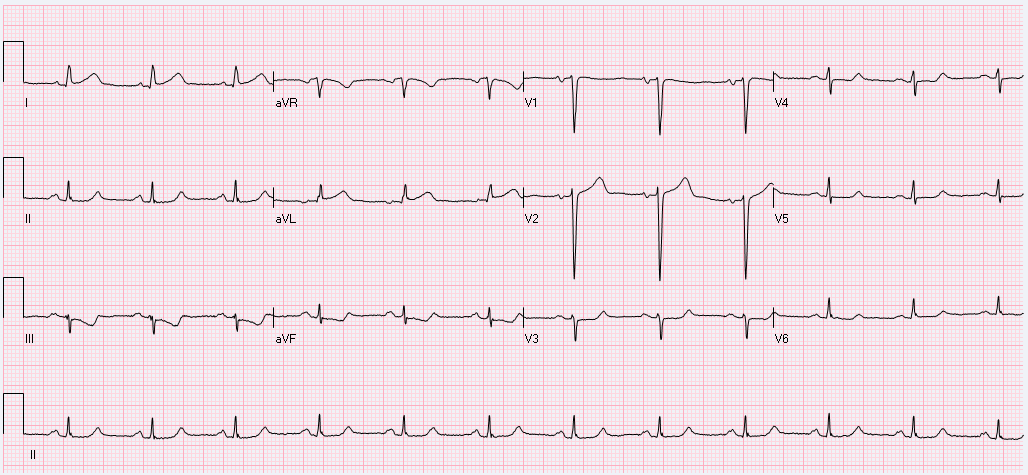 EKG Interpretation: normal sinus rhythm at a rate of 71 with a normal axis. Narrow QRS complexes throughout, normal intervals. Mild ST elevation in I, aVL, and V2. Inverted T wave in III with mild ST depression as well. No previous EKG available for comparison. Discussion: Although this patient does not have an obvious STEMI on their EKG, there is mild elevation in I, aVL and V2 with reciprocal changes in III, a pattern similar to the South African flag. Concern should be high for a high lateral MI which is an area of that is poorly represented by standard EKG lead placement. In this case, the patient had an acute thrombotic occlusion of a diagonal branch of the LAD artery. 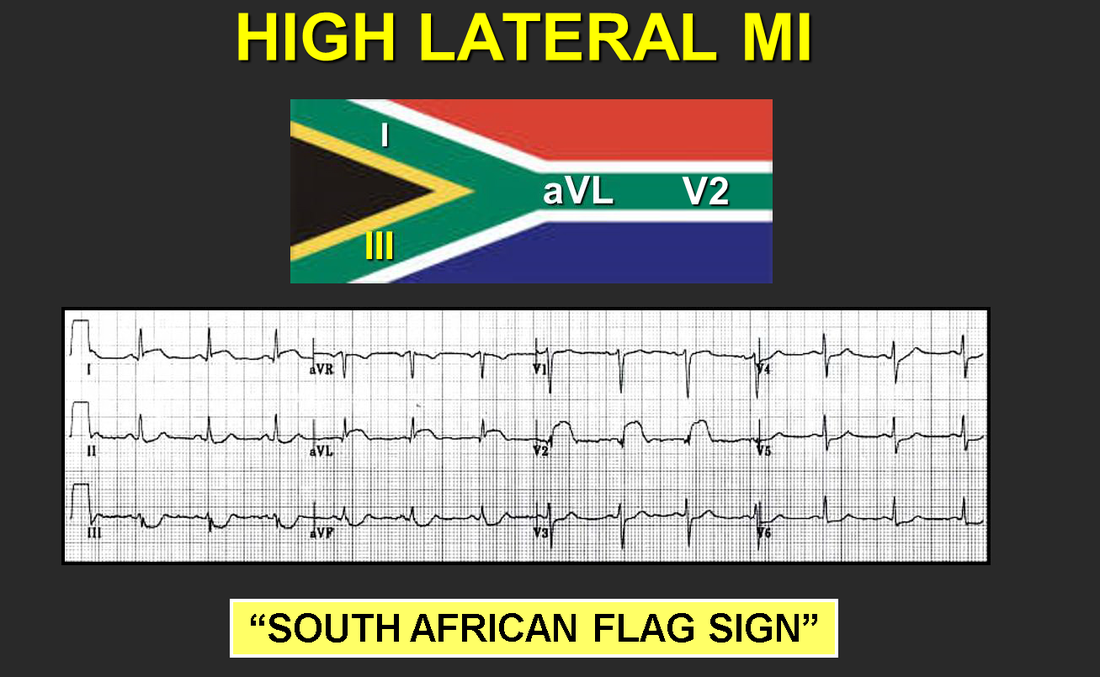 On the initial EKG, the patient has lower voltages in their limb leads as well as V3-V6. Although they don’t have frank ST elevation ≥ 1 mm in any lead other than V2, their mild ST elevation should be concerning given the low(er) QRS voltage. Move one of the V leads higher into the left axilla (2-3 interspaces) to obtain a tracing of the high lateral wall. Make sure to discuss with Cardiology your concern for a potential STEMI despite the lack of qualifying ST elevation.
Management: - Obtain EKG tracing of high lateral wall - Labs including troponins as well as CXR - MONA, heparin - Cardiology consult emphasizing the concern for ST changes in the setting of low QRS voltage - Consider emergent cath for patients with persistent chest pain and persistent ST changes By: Dr. Andrew Godfrey
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
