|
HPI: Middle age male with no significant past medical history presented to the ED with chest pain. Patient was exercising when he developed left-sided chest pain radiating to his left shoulder. Vital signs within normal with initial EKG below: EKG #1: 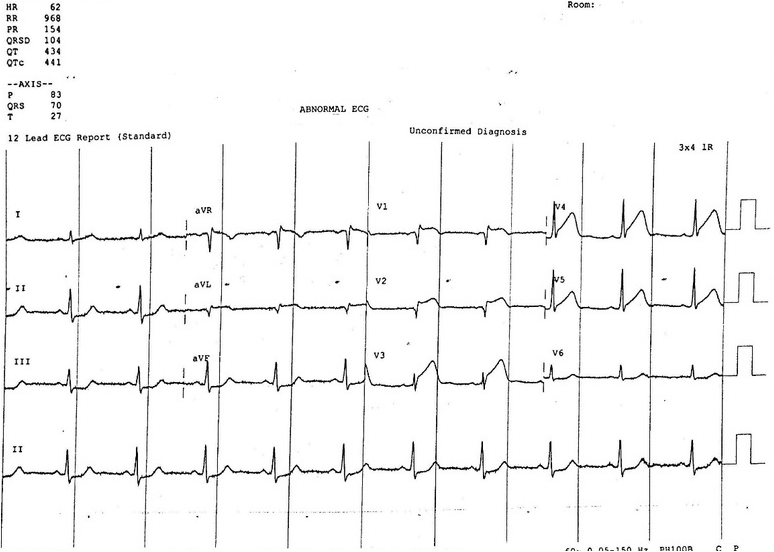 EKG #1 Interpretation: sinus rhythm with normal rate. Normal axis. ST elevation in antero-lateral leads (V1-V5) with reciprocal ST depression in inferior leads (II, III, and aVF). Narrow QRS complex. Borderline prolonged QTc interval. Normal PR interval. EKG findings consistent with acute MI in antero-lateral distribution. Taken for emergent PCI for acute STEMI. Had the following EKG shortly after successful reprefusion and stenting. EKG #2: 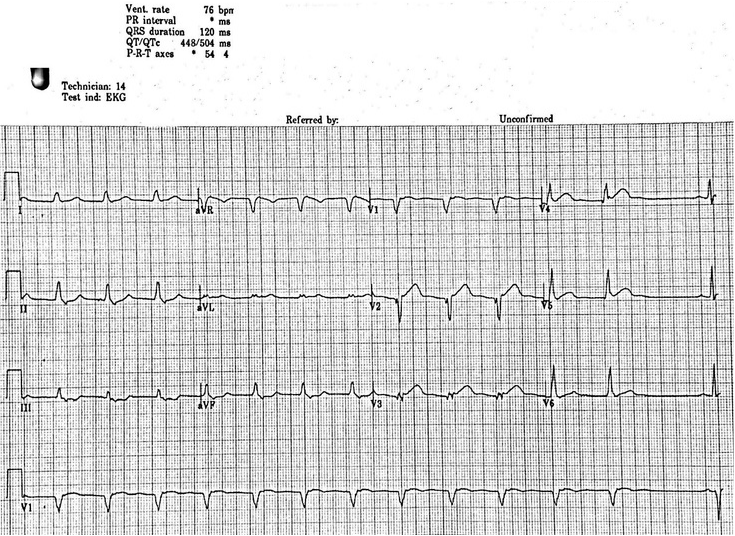 EKG #2 Interpretation: Regular rate at 75, non-sinus rhythm. There are no P waves present in any lead until the last beat of the rhythm strip. Normal axis. ST elevation in antero-lateral leads and reciprocal ST depression in inferior leads is improved from previous EKG. QRS widened. QTc is prolonged at 504ms.
Non-sinus rhythm with widened QRS complex and normal rate in the setting of recent reperfusion is likely accelerated idioventricular rhythm. Discussion: EKG features consistent with accelerated idioventricular rhythm include: 1. Regular rhythm 2. Rate 50-110 bpm 3. QRS greater than 120ms 4. 3 or more ventricular complexes 5. Fusion and capture beats *The rate of a IVR distinguishes it from other rhythms of similar morphology (i.e. non-sinus, wide QRS complex). If rate less than 50 bpm consider a ventricular escape rhythm, if rate greater than 110 bpm consider ventricular tachycardia There are multiple causes of a IVR which include: 1. Reperfusion phase after an acute myocardial infarction (most common) 2. Beta sympathomimetics including isoprenaline or adrenaline 3. Toxicologic causes including digoxin, cocaine, and voltaile anesthetics 4. Electrolyte abnormalities 5. Cardiomyopathy, congenital heart disease, myocarditis 6. ROSC following cardiac arrest Management: -AIVR is usually self-limiting, benign, and does not require any treatment. The underlying cause should be treated, for example correcting electrolytes or reversing toxicologic causes. -In patients who have severe CHF and are dependent on the “atrial kick”, they may benefit from resynchrony. In this case a dose of atropine may be trialed in order to increase sinus rate and potentially improve AV conduction.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
