|
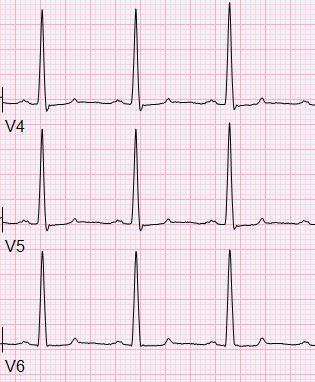
HPI: Patient is a 50 yo F with a history of ESRD s/p failed renal transplant now on hemodialysis who had onset of GI bleeding with associated lightheadedness and hypotension. An EKG was obtained. EKG: 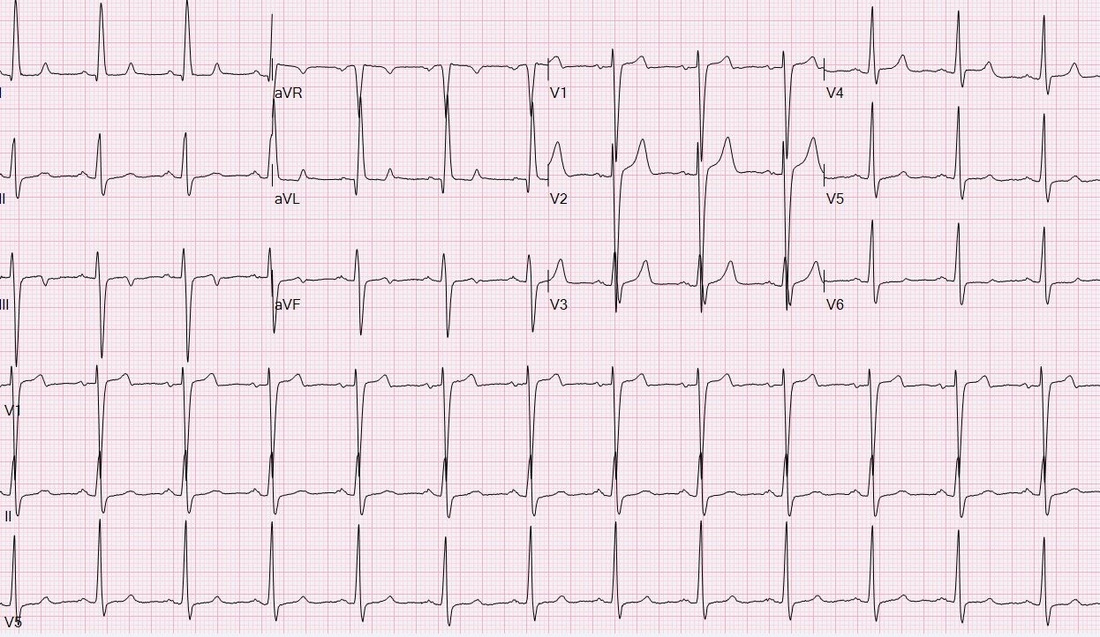 Question: What finding on this EKG warrants further management? EKG Interpretation: Normal sinus rhythm at a rate of 77, normal PR interval, normal QRS, normal axis, LVH (significantly increased voltages), narrow based, peaked T-waves, T-wave inversions in leads III and aVF. Discussion: The narrow based, peaked T-waves present in this patient’s EKG, most evident in leads V3-V4, indicate probable hyperkalemia in this patient who is at risk for elevated potassium given her ESRD. The T-wave abnormalities in this EKG are somewhat subtle, but the narrow, “pinched down” bases of the T-waves should warn you of hyperkalemia. This patient’s potassium level was found to be 6.9 and was appropriately treated. Pro-tip:
 Potassium can be the great imitator on EKGs because it can cause a wide variety of abnormal EKG findings, including (but not limited to): • Peaked T-waves (often the earliest EKG sign of hyperkalemia) • Prolonged PR interval • Loss of P waves • AV block • Broad QRS complexes with abnormal morphology • Sine waves (usually with extremely severe hyperkalemia) 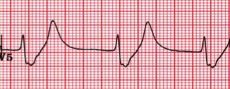 Management:
For patients with ESRD on hemodialysis, dialysis is the definitive treatment for hyperkalemia. Typical management of hyperkalemia (for K>6.0 or EKG changes) includes**: • Calcium (either IV calcium gluconate or calcium chloride), which stabilizes cellular membranes by antagonizing the effect of potassium on membrane potential. Usually reserved for K>7.0 or EKG changes. • Insulin to promote the movement of potassium into cells. • Albuterol and Sodium bicarbonate can also be used to promote the movement of potassium into cells depending on potassium levels. • Kayexalate (Sodium polystyrene sulfonate) can be used to promote potassium elimination from the body, however this has no role in the acute management of hyperkalemia with EKG changes. **Caution in patients with DKA because total body potassium may actually be low and aggressive management of hyperkalemia can result in hypokalemia** By: Krystin Thomas, PGY1 Resources: • Stone, CK. Fluid, Electrolyte, and Acid-Base Emergencies. In Current diagnosis & treatment emergency medicine. 6th ed. New York: McGraw-Hill; 2008. • Burns, E. Hyperkalemia [Web log post] Retrieved August 28, 2015, from http://lifeinthefastlane.com/ecg-library/basics/hyperkalaemia/
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
