|
HPI: 50 y/o male with hx of COPD, heroin use, and recently diagnosed cor pulmonale presents with 3 weeks of lower extremity edema. No chest pain, shortness of breath, or palpitations. An EKG is obtained in the emergency department. 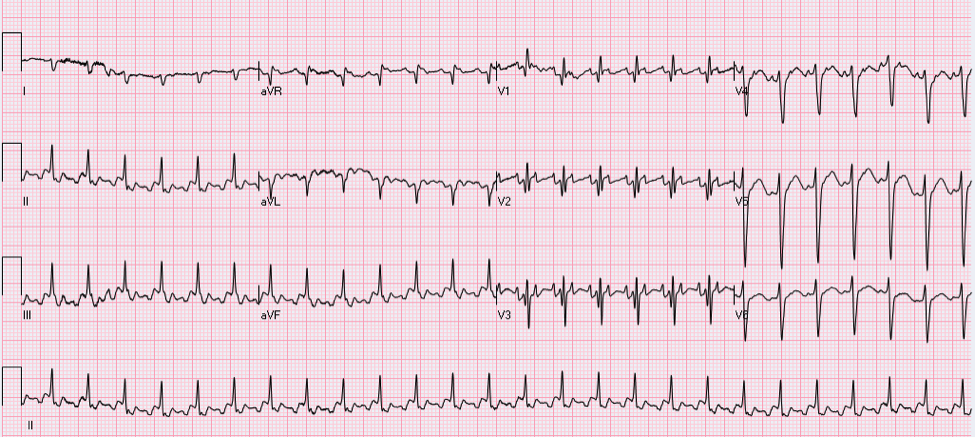 Question: What does this EKG tell you about the etiology of this patient’s lower extremity edema? EKG Interpretation: 2:1 atrial flutter with a rapid ventricular response at a rate of 156, narrow QRS (may appear wide due to buried P-waves), right axis deviation, RBBB. Discussion: The patient presents in 2:1 atrial flutter with a ventricular rate of 156, meaning that the atria are firing at a rate 2 times faster (approximately 312). The extra P-waves give the EKG baseline the typical “sawtooth” appearance of atrial flutter.  Typical characteristics of atrial flutter:
· Regular atrial rate – between 250-350 bpm · Sawtooth flutter waves – directed superiorly and most visible in leads II, III, and aVF · Atrioventricular block – usually at 2:1, but occasionally greater, associated with ventricular rate between 125-175 bpm Pro-tip: If you ever have difficulty distinguishing the buried P-waves of atrial flutter, you can block down the AV node with vagal maneuvers or Adenosine and the slowing of the ventricular rate will unmask the underlying atrial rhythm. Narrow-complex tachycardia at a rate of 130-170: suspect flutter!! Atrial flutter was the cause of this patient’s severe lower extremity edema extending to the scrotum and pre-sacral level. It is not uncommon for patients in atrial flutter to present with edema due the lack of forward flow through the heart secondary to atrial flutter. This patient’s atrial flutter is most likely a result of his severe cor pulmonale, his right atria and ventricle were found to be massively dilated on echocardiogram, predisposing patient to atrial flutter. In general, patients with right heart disease are more likely to get atrial flutter rather than atrial fibrillation, however “where there’s fib, there’s flutter” and these patients can exhibit episodes of a.fib as well. Management: If the patient is stable, the first priority is to achieve ventricular rate control with beta-blockers or nondihydropyridine calcium channel blockers. This patient was given a Diltiazem bolus and then placed on a drip which improved his rate into the 80s, although he was still in 2:1 atrial flutter. Long-term management options for stable patients can be divided into rate control or rhythm control. Rhythm control options: · Cardioversion is an option if patient is known to have been in this rhythm for < 48 hours, if > 48 hours patient requires either: a TEE without evidence of mural thrombus + Heparin or >= 3 weeks of anticoagulation prior to cardioversion (all patients need 4 weeks of anticoagulation post-cardioversion as well) · Catheter ablation for select patient’s (larger right atrium size correlates with lower success rates) Rate control options: · Calcium channel blockers · Beta-blockers By: Dr. Krystin Thomas, MD References: 1. Tintinalli JE. Cardiac Rhythm Disturbances. In: Tintinalli's Emergency Medicine a Comprehensive Study Guide. 7th ed. New York: McGraw-Hill; 2011. 2. Burns, E. Atrial Flutter [Web log post] Retrieved August 15, 2015, from http://lifeinthefastlane.com/ecg-library/atrial-flutter/
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
