|
Clinical context: This is a 20s year-old male who presented to the ED after GSW to the thorax. He lost pulses in transport, and underwent ED thoracotomy, cardiac massage and aortic cross clamping with ROSC, and subsequent ex-lap. He has been in the ICU with complications including respiratory failure, renal failure, hemorrhagic shock, and multiple returns to the operating room for intrabdominal injuries. The following EKG was obtained over the weekend due to ST elevation noted on cardiac telemetry. 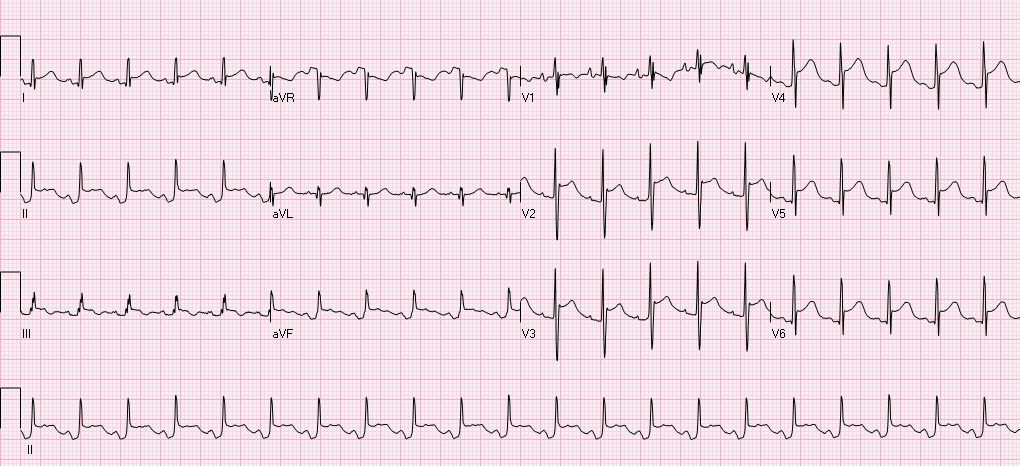 Automated read notes sinus tachycardia, ****ACUTE MI/STEMI****
Let's systematically review this ECG. The ventricular rate is 126, there is a p wave before every QRS - sinus rhythm, QRS is upgoing in I, II - normal axis, PR, QRS intervals appropriate, QTC prolonged at 492, there is ST elevation in I, II, III, aVF, V2-V6 with concomitant PR depressions, reciprocal ST depressions and PR elevations in aVR and V1. This is a classic ECG for PERICARDITIS. The patient subsequently had cardiac ultrasound that demonstrated a small effusion as well. Remember that classic findings of pericarditis include widespread ST elevation and PR depression with reciprocal changes in aVR +/- V1. Life in the fast lane review of pericarditis While there are many causes of pericarditis, this patient has several underlying risk factors including chest trauma, surgery, and possible infection secondary to limited sterility in the emergency setting. While the reported incidence of acute pericarditis after general thoracic surgery is very low, I was not able to identify any recent literature addressing the incidence of pericarditis after ED thoracotomy in patients without penetrating cardiac injuries. In patients with penetrating cardiac injury delayed secondary cardiac injuries and complications occur at at rate of ~50%. Colchicine is noted to be used as pericarditis prophylaxis in major cardiac surgery and transplant, this could be considered in the ED setting, however the logistics and lack of evidence as to how common this complication is could limit benefit. Complications of ED Thoracotomy include:
Upon return to the OR the day after thoracotomy this patient was noted to have ongoing bleeding from internal mammary arteries, but no damage to coronary arteries or other cardiac damage. References: Imazio, M., Gaita, F., LeWinter, M. Evaluation and Treatment of Pericarditis A Systematic Review. JAMA. 2015;314(14):1498-1506. Fallahnejad M., Kutty AC., Wallace HW. Secondary lesion of penetrating cardiac injuries: a frequent complication. Ann Surg. 1980;191(2):228. Alraies MC, AL Jaroudi W, Shabrang C, et al. Clinical features associated with adverse events in patients with post-pericardiotomy syndrome following cardiac surgery. Am J Cardiol. 2014 Nov;114(9): 142630. Keller D, Kulp H, Maher Z, et al. Life after near death: Long term outcomes of Emergency department thoracotomy survivors. J Trauma Acue Care Surg. 2013 May;74(5):1315-20.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
