|
Authored by: Dr. Chrissy Zauner
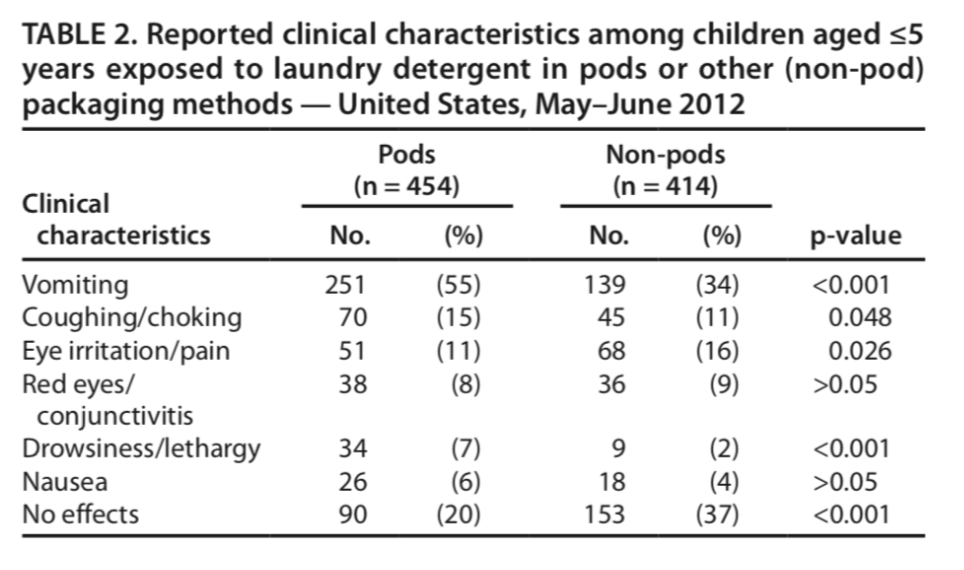
Between January 1st-January 22nd, there were 86 cases of intentional ingestion. As of Saturday, February 10, 2018 a YouTube search produces 81,200 video results, both of videos performing the challenge and those against it. YouTube recently announced it would be pulling videos due to the dangers of exposure. 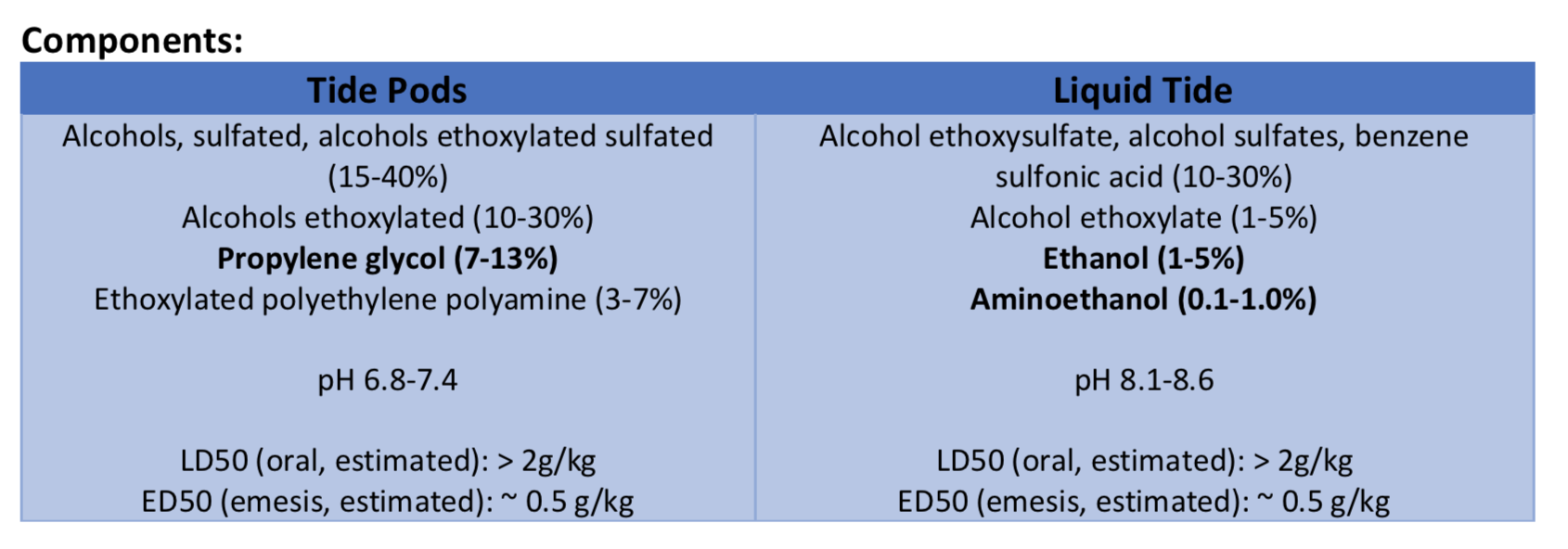 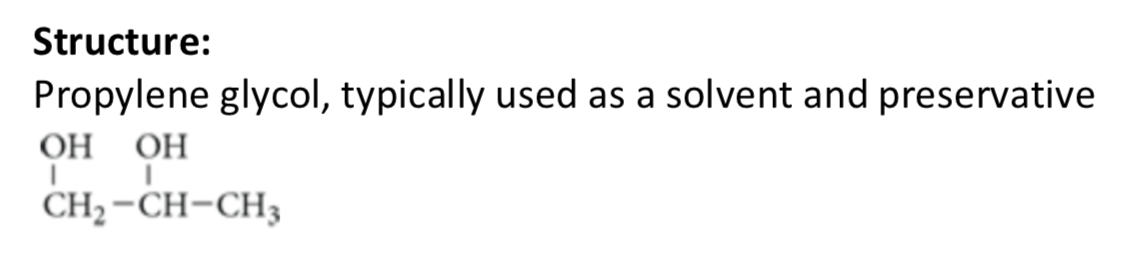 Pharmocology/Pharmokinetics: Unclear overall
Treatment:
References:
0 Comments
Authored by Dr. Enola Okonkwo Introduction Artemether Lumefantrine is an oral medication which is used in treatment of chloroquine resistant uncomplicated malaria. Artemether Lumefantrine falls within the drug class of Artemisinin-based combination therapies which have been found to be highly effective in treating malaria and are substantially less toxic than quinoline antimalarials. Artemisins are derived from a Chinese medicinal herb which comes from the sweet wormwood plant (1). Artemether Lumefantrine, known by the brand name Coartem, is the most widely used artemisinin based combination therapy used in Africa and is one of three medications recommended by the CDC as first line oral treatment for uncomplicated falciparum malaria within the United States (2). Structure 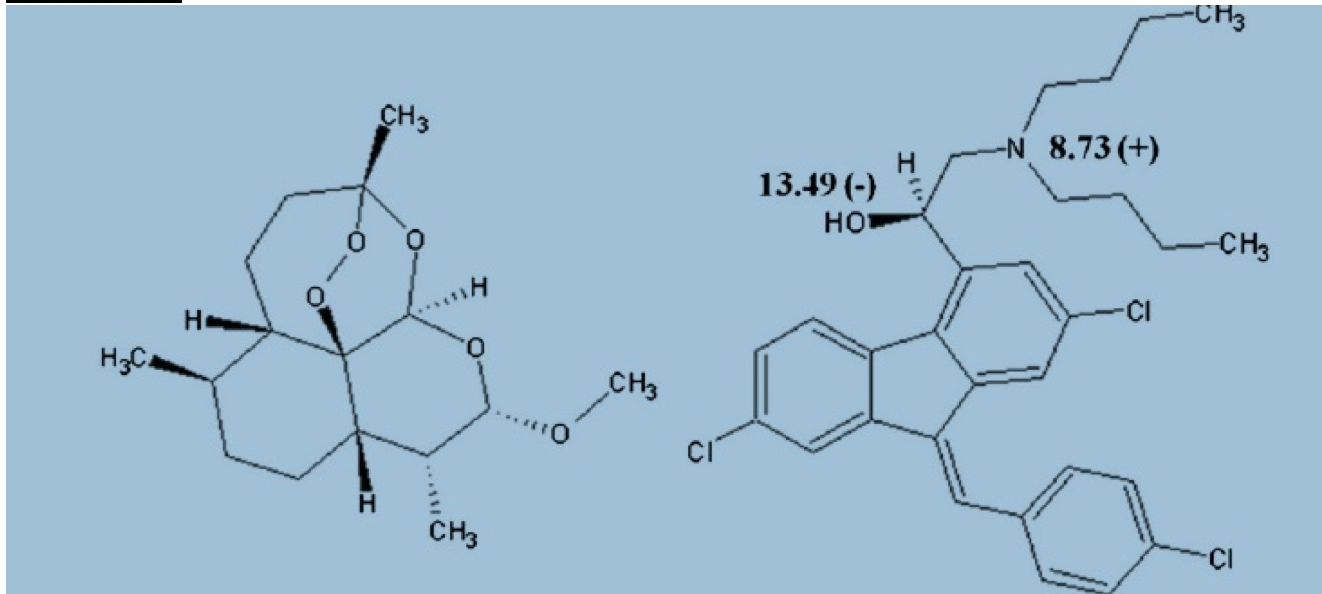 1 tablet = 20mg artemether and 120 mg lumefantrine.
Dosing is weight based. For patients > 35 kg they are taking 4 tablets per dose twice daily for 3 days. Pharmacology/Pharmacokinetics: Absorption/Distribution/Metabolism/Excretion Artemeter is rapidly absorbed. Peak plasma level of artemeter is approximately 2 hours. The half-life after ingestion is 2 hours (4-5). 95% of artemether is protein bound but quickly undergoes metabolism to dihydroartemisin which is approximately 50% protein bound. Half life of dihydroartemisin is also around 2 hours (5). Bioavailability increased 2-3 fold when consumed with food (4). Lumefantrine – Initial absorption at approximately 2 hours. Peak plasma level approximately 6-8 hours. Half life is 4-5 days. It is highly protein bound and has a large volume of distribution. High fat meals significantly increase absorption 16 fold (4). Significant Drug/Drug interactions Numerous theoretic drug interactions have been reported. However, there is scant data available reporting clinical effects of drug interactions. -May enhance QTc prolonging effects -May enhance toxic effects of other antimalarial or HIV medications -May increase serum concentration of antipsychotics -May decrease serum concentration of estrogen related contraceptives -May decrease serum concentration of CYP3A4 Substrates Metabolic Pathways and active metabolites Arthemeter is metabolized by the liver to the active metabolite dihydroartemisinin primarily by CYP3A4/5. Lumefantrine is metabolized by the liver to desbutyl-lumefantrine by CYP3A4. Studies suggest that artemisins inhibit the sarco/endoplasmic reticulum Ca ATPases of the malaria parasite causing rapid reduction in the parasite (6-7). The mechanism of lumefantrine is unknown but both agents inhibit nucleic acid and protein synthesis. Artemether rapidly kills the majority of the parasite and lumefantrine goes on to kill the residual remaining parasite (4-5). Mechanism of Toxicity Artemether Lumefantrine has been extensively used for the treatment of malaria and appears to have an excellent safety profile. There are no reported overdoses or intentional ingestions. There has been no evidence of significant systemic or local toxicity reported in any large human study (1, 20-21). However, there is animal data and a few small human studies and case reports which suggest neurotoxicity and QT prolongation are possible toxic effects of artimisinins (14). Neurotoxicity was especially common in animal studies both clinically and histologically (8-10, 14). In vitro studies have postulated that neurotoxicity results secondary to ATP depletion of neurons and free radical generation created by the breakdown of artemisins (Schmuck 2002, Smith 1998) . Toover et. el wrote a review article cautioning that neurotoxic effects may also occur in humans more frequently than previously thought, though many critics viewed their review as bias (8, 13). There are a small number of case reports within humans suggesting that artemisins contributed to neurologic symptoms such as anxiety, tremor, and ataxia (8, 15-16). A small study looking at construction workers treated with arthemeter suggested that individuals had hearing loss following the administration of artemether (17). Obviously, this study is limited by a serious potential confounder and attempts to reproduce these results have failed (18). One case report of delayed hemolytic anemia, not thought to be related to malaria was reported (19). Clinical Toxicity Given patients taking artemether lumefantrine have malaria, it is difficult to distinguish between symptoms caused by the disease state of malaria versus symptoms which may be attributed to medication toxicity. Clinical toxicity appears to be very rare or possibly underreported. A large review of 188 studies including over 9,000 patients found no serious clinical toxicity (21). This review article used methodology similar to Cochrane review and reported transient neutropenia in 1.3%, reticulocytopenia (0.6%), elevated liver enzymes (0.9%), and transient bradycardia and prolonged QT (1.1%). The most common side effects reported were gastrointestinal. The authors conclude that Artemether Lumefantrine is a safe and efficacious drug. Common adverse events (4, 20-21) Abdominal pain Anorexia Vomiting Diarrhea Headache dizziness. Pruritis and Rash < 2% Laboratories No specific toxicology labs are available Management of Toxicity No accepted recommendations regarding toxicity given the scarcity of data suggesting toxicity. Below are general recommendations based off of literature review: Avoid concurrent use of additional antimalarial medications Use caution administering additional drugs which can prolong QT Use caution in hypokalemia and replete electrolytes as needed Use caution in patients with prolonged QT Obtain EKG as screening for arrhythmia References: 1. Hien, T. T., White, N. J., & White. (1993). Qinghaosu. The Lancet, 341(8845), 603–608. https://doi.org/10.1016/0140-6736(93)90362-K 2. Center for Disease Control. (2009). Guidelines for treatment of malaria in the United States. Treatment Table Update, May, (770), 855–857. Retrieved from http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Guidelines+for+Treatment+of+Malaria+in+the+United+States#1 3. Amin, N. C., Fabre, H., Blanchin, M.-D., Montels, J., & Aké, M. (2013). Determination of artemether and lumefantrine in anti-malarial fixed-dose combination tablets by microemulsion electrokinetic chromatography with short-end injection procedure. Malaria Journal, 12, 202. https://doi.org/10.1186/1475-2875-12-202 4. Waning, B., & Montange, M. (2015). Access Pharmacy. Retrieved from http://accesspharmacy.mhmedical.com/content.aspx?bookid=438§ionid=40428529 5. White, N. J., Van Vugt, M., & Ezzet, F. (1999). Clinical pharmacokinetics and pharmacodynamics of artemether-lumefantrine. Clinical Pharmacokinetics. Adis International Ltd. https://doi.org/10.2165/00003088-199937020-00002 6. Krishna, S., Pulcini, S., Moore, C. M., Teo, B. H. Y., & Staines, H. M. (2014, January). Pumped up: Reflections on PfATP6 as the target for artemisinins. Trends in Pharmacological Sciences. https://doi.org/10.1016/j.tips.2013.10.007 7. Eckstein-Ludwig, U., Webb, R. J., Van Goethem, I. D. A., East, J. M., Lee, A. G., Kimura, M., … Krishna, S. (2003). Artemisinins target the SERCA of Plasmodium falciparum. Nature, 424(6951), 957–961. https://doi.org/10.1038/nature01813 8. Toovey, S. (2006, October 10). Are currently deployed artemisinins neurotoxic? Toxicology Letters. https://doi.org/10.1016/j.toxlet.2006.06.001 9. Genovese, R. F., Newman, D. B., Li, Q., Peggins, J. O., & Brewer, T. G. (1998). Dose-dependent brainstem neuropathology following repeated arteether administration in rats. Brain Research Bulletin, 45(2), 199–202. https://doi.org/10.1016/S0361-9230(97)00339-0 10. Petras, J. M., Young, G. D., Bauman, R. A., Kyle, D. E., Gettayacamin, M., Webster, H. K., … Brewer, T. G. (2000). Arteether-induced brain injury in Macaca mulatta. I. The precerebellar nuclei: The lateral reticular nuclei, paramedian reticular nuclei, and perihypoglossal nuclei. Anatomy and Embryology, 201(5), 383–397. https://doi.org/10.1007/s004290050326 11. Schmuck, G., Roehrdanz, E., Haynes, R. K., & Kahl, R. (2002). Neurotoxic mode of action of artemisinin. Antimicrobial Agents and Chemotherapy, 46(3), 821–827. https://doi.org/10.1128/AAC.46.3.821-827.2002 12. Smith, S. L., Maggs, J. L., Edwards, G., Ward, S. A., Park, B. K., & McLean, W. G. (1998). The role of iron in neurotoxicity: a study of novel antimalarial drugs. Neurotoxicology, 19(4–5), 557–559. 13. Toovey, S. (2006, October 10). Are currently deployed artemisinins neurotoxic? Toxicology Letters. https://doi.org/10.1016/j.toxlet.2006.06.001 14. Brewer, T. G., Peggins, J. O., Grate, S. J., Petras, J. M., Levine, B. S., Weina, P. J., … Schuster, B. G. (1994). Neurotoxicity in animals due to arteether and artemether. Transactions of the Royal Society of Tropical Medicine and Hygiene, 88, 33–36. https://doi.org/10.1016/0035-9203(94)90469-3 15. Miller, L. G., & Panosian, C. B. (1997). Ataxia and slurred speech after artesunate treatment for falciparum malaria. New England Journal of Medicine, 336(18), 1328. https://doi.org/10.1056/NEJM199705013361818 16. Franco-Paredes, C., Dismukes, R., Nicolls, D., & Kozarsky, P. E. . (2005). Neurotoxicity Due to Antimalarial Therapy Associated with Misdiagnosis of Malaria. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 40(11), 1710–1711. https://doi.org/10.1086/430180 17. Toovey, S. (2006). A case-control auditory evaluation of patients treated with artemether-lumefantrine. American Journal of Tropical Medicine and Hygeine 74, 939-940. 18. Hutagalung, R., Htoo, H., Nwee, P., Arunkamomkiri, J., Zwang, J., Carrara, V. I., … Nosten, F. (2006). A case-control auditory evaluation of patients treated with artemether-lumefantrine. American Journal of Tropical Medicine and Hygiene, 74(2), 211–214. https://doi.org/74/2/211 [pii] 19. Hasegawa, C., Kudo, M., Maruyama, H., Kimura, M. (2017). Severe delayed haemolytic anaemia associated with artemether-lumefantrine treatment of malaria in a Japanese traveler. Journal of Infection and Chemotherapy. In press. https://doi.org/10.1016/j.jiac.2017.10.008 20. Alkadi, H. O. (2007, November). Antimalarial drug toxicity: A review. Chemotherapy. https://doi.org/10.1159/000109767 21. Ribeiro, I. R., & Olliaro, P. (1998). Safety of artemisinin and its derivatives. A review of published and unpublished clinical trials. Medecine Tropicale : Revue Du Corps de Sante Colonial, 58(3 Suppl), 50–53. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=10212898 Authored by Dr. Kyle Roedersheimer Introduction to ADHD
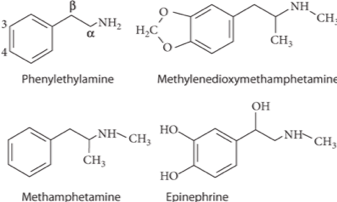
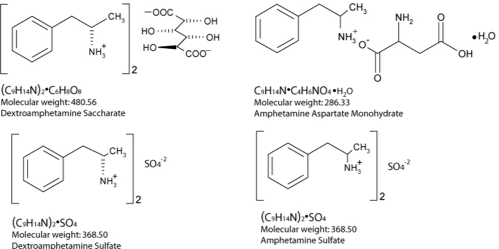
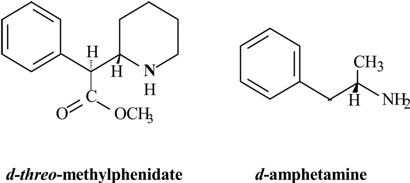
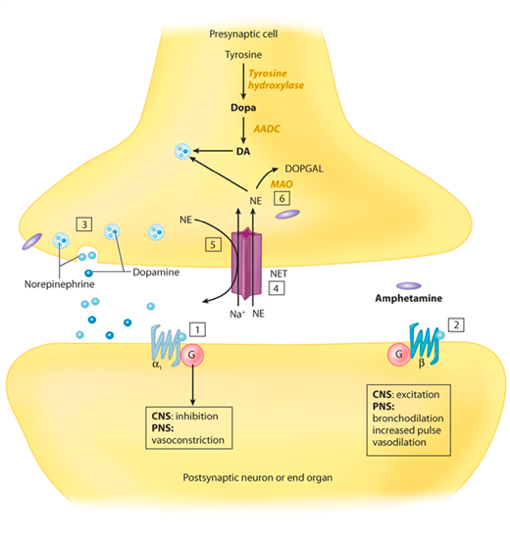
History of Amphetamines
Psychostimulants
Mechanism of action
Pharmacology/Pharmacokinetics:
Therapeutic levels
Significant Drug/Drug Interactions
Metabolic Pathways and active metabolites
Diagnostic Testing and Laboratories
Treatment/Management
What is Stuttering? What causes it?
Multiple Case Reports Discussing Stuttering Associated with ADHD Medications
References
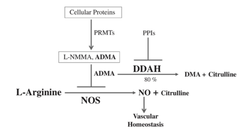
Authored By: Meredith Binford Background: Proton pump inhibitors (PPIs) inhibit H+K+ATPase proton pumps in the stomach to reduce acid excretion. Among the most frequently prescribed drugs worldwide and are generally well tolerated. Now they are available for long-term use without medical supervision. Often prescribed to circumvent GI side effects from dual antiplatelet agents used for cardiovascular disease secondary prevention. However recent observational studies have linked PPI use to increased cardiovascular risk (MI and stroke) even in patients not taking antiplatelet agents. Mechanism: -impair lysosomal acidification and enzyme activity -accelerate telomere erosion -speed endothelial aging as manifested by impaired cell perforation and angiogenesis -impair the NO synthase pathway though asymmetric dimethylarginine (ADMA)
3 recent articles investigate PPIs and risk of stroke: 1. A large retrospective study from the Taiwan National Health Insurance Database studied whether PPI use alone could be associated with first time ischemic stroke. In a propensity score matched analysis (400,000 patients) over 120 days PPI use was associated with a higher risk of hospitalization due to ischemic stroke with hazard ratio of 1.36 (95% CI 1.14-1.62, P=0.001). In subgroup analysis, the risk was more prominent in those less than 60 years of age but gender, prior MI, diabetes, hypertension, use of antiplatelet agents or NSAIDs, or types of PPI did not have an influence on the risk. In the nested case-control analysis (30,000 patients), the adjusted odds ratios for PPI use were 1.77 (95% CI 1.45-2.17, P<0.001) within 30 days and 1.65 (95% CI 1.31-2.08, P<0.001) 31 to 90 days before ischemic stroke. The proportions of H2 blocker users and non users were comparable before the event. One of the major arguments against the association is confounding by indication for PPI use as PPIs are used over H2 blockers in the presence of more severe acid related GI disorders. Other uncorrected confounders include obesity, lack of exercise, smoking, compliance with hypertension treatment, diabetes, hyperlipidemia, other medical illnesses. Also limited by 120 day follow up which may have masked confounders of PPI use. 2. Danish registry of people who underwent elective EGD (215,000 patients) was analyzed in a time varying design to asses dose response effects on hazard ratios as well as in a baseline treatment design to show impact of long term use on risks of first time stroke and MI. Current PPI exposure was associated with significantly higher rates of both ischemic stroke with hazard ratio of 1.13 (95% CI 1.08-1.19) and MI with hazard ratio of 1.31 (95% CI 1.23-1.39) after adjusting for age, sex, comorbidities and concomitant medications. High dose PPI was associated with increased rates of ischemic stroke with hazard ratio of 1.31 (95% CI 1.21-1.42) and MI with hazard ratio of 1.43 (95% CI 1.30-1.57). H2 blockers were not significantly associated with ischemic stroke or MI. Long-term PPI users had a 29% greater absolute risk of ischemic stroke and a 36% greater absolute risk of MI within six months period. One limitation is confounding that PPI identifies unhealthy individuals. When estimating impact of smoking habit, obesity, and exercise the net confounding bias was between 3.8 and 4.1% which reduced the hazard ratio to 1.08 for ischemic stroke and 1.26 for MI. Also concern of a lead in bias as subjects were likely exposed to PPI therapy before EGD. 3. Analysis from the Nurses Health Study and the Health Professionals Follow Up Study (950,000 person years) observed an association between regular PPI use and risk of ischemic stroke in age-adjusted models and multivariate models adjusting for known risk factors for ischemic stroke that was consistent with findings of prior reports. However additional adjustment for factors that may be associated with initiation and continuation of PPI therapy including history of peptic ulcer disease, GERD, GI bleeding and prior H2 blocker use substantially attenuated the association. They found that participants who were regular PPI users at baseline tended to have higher rates of chronic medical conditions including prior history of hypertension, hyperlipidemia, CAD, diabetes, as well as lower levels of physical activity expenditure. Among women, regular PPI users were more likely to have a higher BMI and a prior history of menopausal hormonal use. Association of PPI use with ischemic stroke may be due to residual confounding by factors associated with the indication for PPI use, for example metabolic syndrome. Conclusion: There is a plausible biological mechanism to explain the association of PPIs with increased cardiovascular risk. Large retrospective studies show association especially with longer use and higher dose PPI. However there is concern of confounding as may be related to more unhealthy patients using PPIs. References: Sehested, TSG et al. Long term use of proton pump inhibitors, dose-response relationship and associated risk of scheming stroke and myocardial infarction. Journal Internal Medicine 2017, doi: 10.1111/joim.12698. Nguyen LH, Lochhead P, Joshi AD, Cao Y, Ma W, Khalili H, Rimm EB, Rexrode KN< Chan AT. No significant association between proton pump inhibitor use and risk of stroke after adjustment for lifestyle factors and indication. Gastroenterology 2018, doi: 10.1053/j.gastro.2017.12.006. Wang Y-F, Chen Y-T, Luo J-C, Chen T-J, Wu J-C, Wang S- J. Proton-pump inhibitor use and the risk of first-time ischemic stroke in the general population: a nationwide population-based study. Am J Gastroenterol 2017; 112: 1– 10. Yepuri G, Sukhovershin R, Nazari-Shafti TZ, Petrascheck M, Ghebre YT, Cooke JP. Proton pump inhibitors accel- erate endothelial senescence. Circ Res 2016; 118: e36–42. Ghebremariam YT, Lependu P, Lee JC et al. Unexpected effect of proton pump inhibitors: elevation of the cardiovascular risk factor asymmetric dimethylarginine. Circulation 2013; 128: 845–53. Cooke JP. Asymmetrical dimethylarginine: the u€ber marker? Circulation 2004; 109: 1813–9. Authored by Dr. Natalie Wood
Uses: -The flesh of the fruit consists of an edible, white pulp , some fiber, and a core of indigestible, black seeds. Used in foods -eaten as dessert -smoothies, fruit juice drinks -candy -sorbets and ice cream flavoring -Traditional medicinal uses for diarrhea, liver disease, heart disease, intestinal parasites, diabetes, and cancer. -Pesticides, insecticides and topical insect repellant in latin america -shampoos for treating lice and ticks
-This is exceptionally frequent compared to epidemiological data from European countries where atypical parkinsonism accounts for only approximately 5% of all cases - A higher proportion of patients with atypical parkinsonism (consumed soursop fruit 97%; consumed herbal tea 83%) than patients with Parkinson’s disease (fruit 59%; herbal tea 18%) or control with no Parkinson symptoms (fruit 60%; herbal tea 43%). -When directly injecting rats for one month with the estimated amounts of annonacin ingested in a year by eating one fruit daily, this induced neurodegeneration in the basal ganglia and mesencephalon (Champy et al., 2004) -As an indication of its potential toxicity, an adult who consumes one fruit or can of nectar a day is estimated to ingest over 1 year the amount of annonacin that induced brain lesions in rats receiving purified annonacin by intravenous infusion. -Multiple studies showing toxicity in vitro to dopaminergic neurons -Cultured neurons treated with low doses of annonacin exhibit hallmarks of tauopathy, including increased tau concentration, tau hyperphosphorylation, cell death and somatodendritic redistribution of hyperphosphorylated tau which is that same pathophysiology of progressive supranuclear palsy. -Studied as a cytotoxic agent for use in cancer chemotherapy -Extract from the seeds and leaves have IC50 comparable to doxorubicin at .57μg/mL (seed) and .36μg/mL (leaves) compared to .11μg/mL (doxorubicin) in leukemia cells. -Mechanism of action is via annonacin, the acetogenin causing mitochondrial membrane potential disruption. It inhibits NADH dehydrogenase on Complex I of the electron transport chain. Creates reactive O2 species that can damage DNA and other components of mitochondria -Annona muricata leaf extract reduced the tumor's size and weight, showed anti-metastatic features, and induced apoptosis in vitro and in vivo of the 4 T1 breast cancer cell lines. Furthermore, it decreased the level of nitric oxide and malondialdehyde in tumor while also increased the level of white blood cell, T-cell, and natural killer cell population. 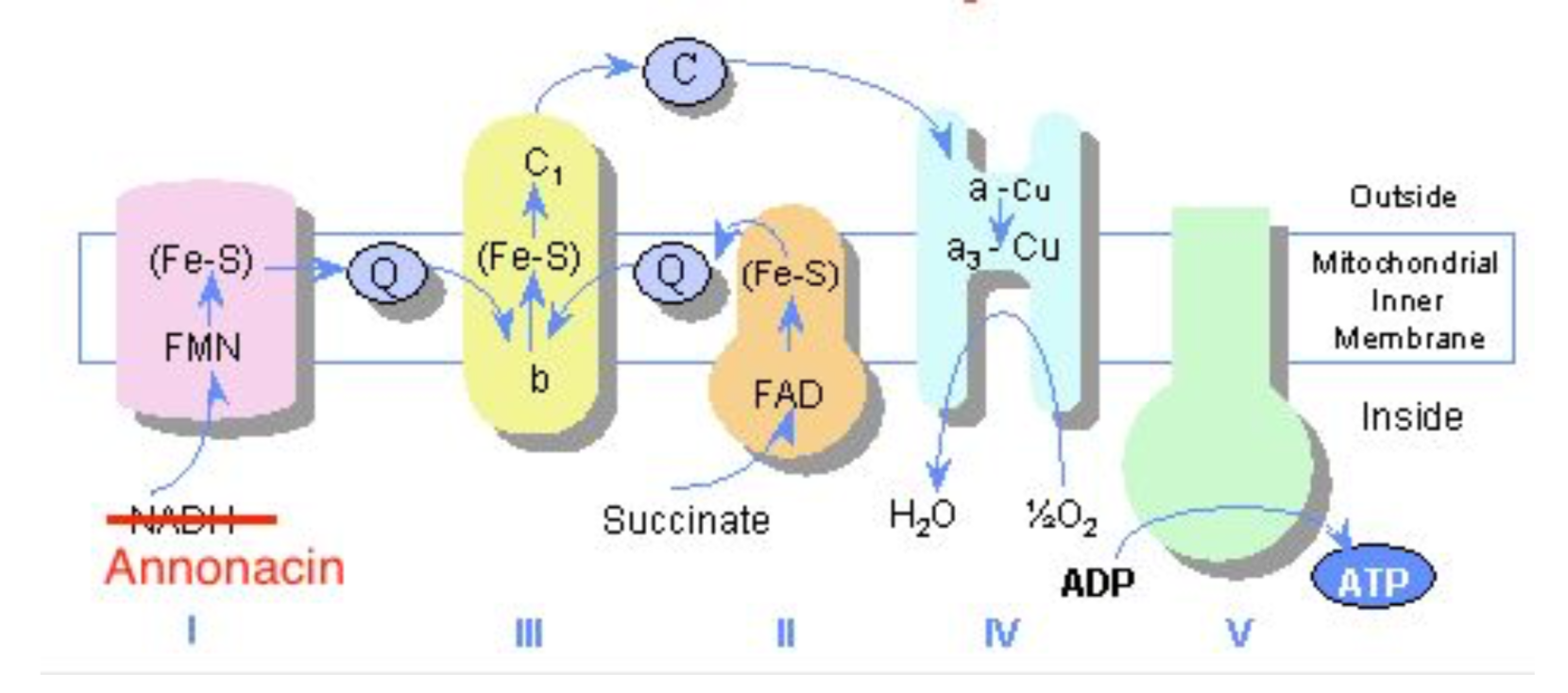 Pharmacology -LD 50 >2g/kg -In IV administration to Rats 3800 and 7600 μg/kg daily caused neurodegeneration over a period of 28 days -it appears that chronic consumption causes the neurodegeneration Presentation -Levodopa resistant parkinsonism similar to progressive supranuclear palsy -PSP presents with loss of balance, bradykinesia, rigidity, problems controlling eye movements, issues with speech and swallowing -Patients in Guadaloupe: -early postural instability -supranuclear oculomotor dysfunction -greater frequency of patients with tremor as compared to typical PSP -greater frequency of patients with hallucinations as compared to typical PSP Laboratories -no laboratory evidence of annonacin toxicity -annonacin can be identified in brain neurons on autopsy Treatment/Management -stop ingestion of soursop -poor response to levodopa or other parkinson’s treatment agents Resources Caparros-Lefebvre, Dominique, Nicolas Sergeant, Andrew Lees, Agnes Camuzat, Susan Daniel, Annie Lannuzel, Alexis Brice, Eduardo Tolosa, Andre Delacourte, and Charles Duyckaerts. "Guadeloupean parkinsonism: a cluster of progressive supranuclear palsy-like tauopathy." Brain 125.4 (2002): 801-11. Web. 9 July 2017. Champy, Pierre, Alice Melot, Vincent Guérineau Eng, Christophe Gleye, Djibril Fall, Gunter U. Höglinger, Merle Ruberg, Annie Lannuzel, Olivier Laprévote, Alain Laurens, and Reynald Hocquemiller. "Quantification of acetogenins inAnnona muricata linked to atypical parkinsonism in guadeloupe." Movement Disorders 20.12 (2005): 1629-633. Web. 9 July 2017. Clement, Yuri N., Varune Mahase, Annelise Jagroop, Kelly Kissoon, Aarti Maharaj, Prashant Mathura, Chrys Mc Quan, Divya Ramadhin, and Cherrista Mohammed. "Herbal remedies and functional foods used by cancer patients attending specialty oncology clinics in Trinidad." BMC Complementary and Alternative Medicine 16.1 (2016): n. pag. Web. 09 July 2017. Coria-Téllez, Ana V., Efigenia Montalvo-Gónzalez, Elhadi M. Yahia, and Eva N. Obledo-Vázquez. "Annona muricata: A comprehensive review on its traditional medicinal uses, phytochemicals, pharmacological activities, mechanisms of action and toxicity." Arabian Journal of Chemistry (2016): n. pag. Web. 9 July 2017. Esposti, M. Degli, A. Ghelli, M. Ratta, D. Cortes, and E. Estornell. "Natural substances (acetogenins) from the familyAnnonaceaeare powerful inhibitors of mitochondrial NADH dehydrogenase (Complex I)." Biochemical Journal 301.1 (1994): 161-67. Web. 9 July 2017. Kuete, Victor, Joachim K. Dzotam, Igor K. Voukeng, Aimé G. Fankam, and Thomas Efferth. "Cytotoxicity of methanol extracts of Annona muricata, Passiflora edulis and nine other Cameroonian medicinal plants towards multi-factorial drug-resistant cancer cell lines." SpringerPlus 5.1 (2016): n. pag. Web. Salama, Mohamed, and Oscar Arias-Carrión. "Natural toxins implicated in the development of Parkinson’s disease." Therapeutic Advances in Neurological Disorders 4.6 (2011): 361-73. Web. 9 July 2017. Lannuzel, A., G. U. Hoglinger, S. Verhaeghe, L. Gire, S. Belson, M. Escobar-Khondiker, P. Poullain, W. H. Oertel, E. C. Hirsch, B. Dubois, and M. Ruberg. "Atypical parkinsonism in Guadeloupe: a common risk factor for two closely related phenotypes?" Brain 130.3 (2007): 816-27. Web. 9 July 2017. Soursop . N.p., n.d. Web. 09 July 2017.
|



| Background Omeprazole
|  |
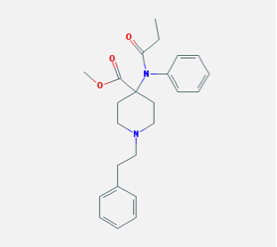
| Methadone -µ opioid receptor agonist -variable oral bioavailability, 36-100% -onset 30min-1hr, time to peak ~4hrs -85-90% protein bound -metabolized by 2B6, 2C19, 2D6 (minor), substrate of 3A4 -excreted in urine, feces; T1/2 24-36 hours -usual formulation is methadone hcl, pka 8.4 (weak base) |  |
Likely mechanism of enhanced effect
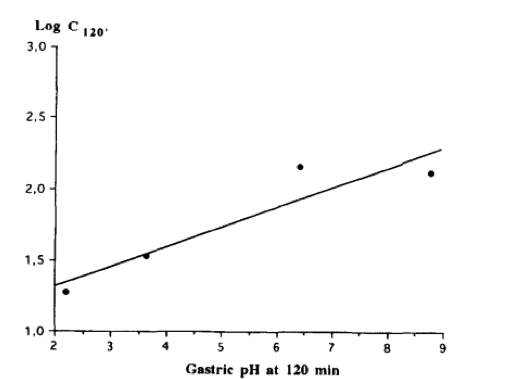
By increasing gastric pH, the absorption of methadone is increased
Angeles-Carlos, et al. (2001):
-Omeprazole 2mg/kg iv 2hr prior to methadone
-rate of absorption faster (k(01) = 0.31 +/- 0.04 min(-1) vs 0.05 +/- 0.007 min(-1)
-peak plasma concentration greater (197.41 +/- 33.70 versus 83.54 +/- 7.97 ng/mL)
-time to reach Cmax shorter (11.23 +/- 1.32 versus 39.18 +/- 1.74 min)
-however, no significant effect on analgesia as assessed by tail twitch testing
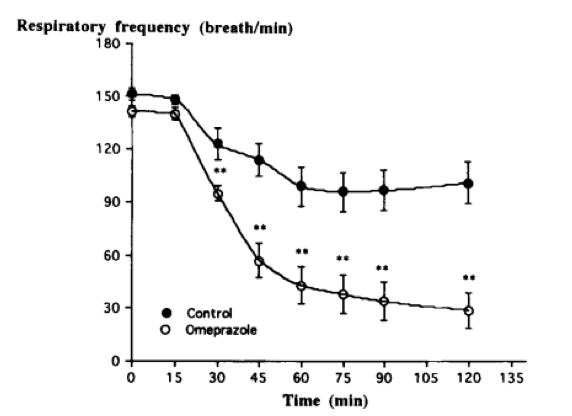
DeCastro, et al. (1996):
Omeprazole 2mg/kg PO with methadone 5mg/kg PO in rats
-Cmax 156 vs 51 ngml-1
-significant differences in respiratory depression, arterial pCO2
-replicated with HCO3 and acidic methadone solution
By increasing gastric pH, the absorption of methadone is increased
Angeles-Carlos, et al. (2001):
-Omeprazole 2mg/kg iv 2hr prior to methadone
-rate of absorption faster (k(01) = 0.31 +/- 0.04 min(-1) vs 0.05 +/- 0.007 min(-1)
-peak plasma concentration greater (197.41 +/- 33.70 versus 83.54 +/- 7.97 ng/mL)
-time to reach Cmax shorter (11.23 +/- 1.32 versus 39.18 +/- 1.74 min)
-however, no significant effect on analgesia as assessed by tail twitch testing
DeCastro, et al. (1996):
Omeprazole 2mg/kg PO with methadone 5mg/kg PO in rats
-Cmax 156 vs 51 ngml-1
-significant differences in respiratory depression, arterial pCO2
-replicated with HCO3 and acidic methadone solution
 |  |
Other potential mechanisms
Inhibition of P-glycoprotein
-Rodriguez, et al. (2004): Methadone cleared from CNS via P-glycoprotein
-Administration of valspodar, a P-gp inhibitor, increased analgesic effect of methadone in rats
three-fold
-Pauili-Magnus, et al. (2001): omeprazole, lansoprazole, pantoprazole inhibit P-glycoprotein
-used digoxin as P-glycoprotein substrate
-no studies directly observing effect on methadone
Inhibition of CYPC19
-Liu, et al. (2005): omeprazole strongly inhibits CYPC19 in vitro
-unlikely to impact methadone metabolism significantly given difference in T1/2
Inhibition of P-glycoprotein
-Rodriguez, et al. (2004): Methadone cleared from CNS via P-glycoprotein
-Administration of valspodar, a P-gp inhibitor, increased analgesic effect of methadone in rats
three-fold
-Pauili-Magnus, et al. (2001): omeprazole, lansoprazole, pantoprazole inhibit P-glycoprotein
-used digoxin as P-glycoprotein substrate
-no studies directly observing effect on methadone
Inhibition of CYPC19
-Liu, et al. (2005): omeprazole strongly inhibits CYPC19 in vitro
-unlikely to impact methadone metabolism significantly given difference in T1/2
Take home message
-Good theoretical basis for potential interaction between omeprazole and methadone via enhanced absorption with increased gastric pH
-Weaker theoretical basis for interaction via P-glycoprotein and CYP enzyme inhibition
-Never demonstrated in humans in experimental setting
-Good theoretical basis for potential interaction between omeprazole and methadone via enhanced absorption with increased gastric pH
-Weaker theoretical basis for interaction via P-glycoprotein and CYP enzyme inhibition
-Never demonstrated in humans in experimental setting
References:
National Center for Biotechnology Information. PubChem Compound Database; CID=4095, https://pubchem.ncbi.nlm.nih.gov/compound/4095 (accessed Nov. 14, 2017).
National Center for Biotechnology Information. PubChem Compound Database; CID=4594, https://pubchem.ncbi.nlm.nih.gov/compound/4594 (accessed Nov. 14, 2017).
Carlos MA, DuSouich P, Carolos R, Suarez E, Lukas JC, Calvo R. Effect of omeprazole on oral and intravenous RS-methadone pharmacokinetics and pharmacodynamics in the rat. Journal of Pharmacologic Science 200
DeCastro J, Aguirre C, Rodriguez-sasiain JM, Gomez E, Garrido MJ, Calvo R. The effect of changes in gastric pH induced by omeprazole on the absorption and respiratory depression of methadone. (1996). Biopharmaceutics & Drug Disposition, 1996(17);551-63
Rodriguez M, Ortega I, Soengas I, Suarez E, Lukas JC, Calvo R. Effect of P-glycoprotein inhibition and brain distribution in the rat. (2004) Journal of Pharmacy and Pharmacology. Mar; 56(3):367-74.
Pauli-Magnus C, Rekersbrink S, Klotz U, Fromm M. Interaction of omeprazole, lansoprazole, and pantoprazole with P-glycoprotein. (2001). Naunyn-Schmiedeberg’s Archives of Pharmacology 364(6); 551-57.
Liu KH, Kim MJ, Shon JH, Moon YS, Seol SY, Kang W, Cha IJ, Shin JG. Stereoselective inhibition of cytochrome P450 forms by lansoprazole and omeprazole in vitro. (2005). Xenobiotica Jan;35(1):27-38.
- Introduction
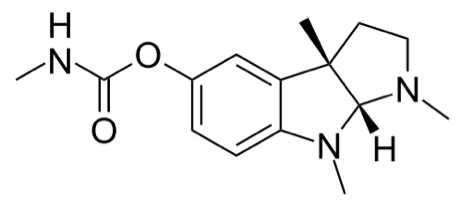
- Naturally-occuring plant-derived alkaloid; is a carbamate that reversibly inhibits cholinesterases in the PNS and CNS
- Is a tertiary amine à allows CNS penetration (where the quaternary amine structure of neostigmine and pyridostigmine limits CNS penetration)
- Used to treat anticholinergic effects of numerous medications and toxins incluiding, TCAs and phenothiazines
- Single study found to address use as a diagnostic tool in suspected anticholinergic syndrome
- Mechanism of action:
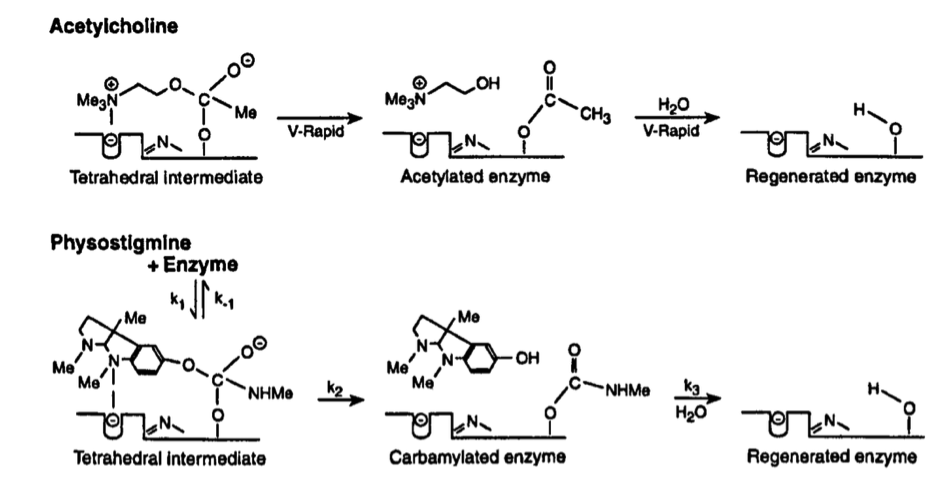
- Reversibly binds to acetylcholinesterase
- Is metabolized by acetylcholinesterase. While the time to hydrolysis of acetylcholine is 150msec, the half-life to hydrolysis in physostigmine is 15-30 minutes. Result is active acetylcholine in the synapse for a prolonged duration
- Reversibly binds to acetylcholinesterase
- Absorption: Poor oral bioavailability - 5-12%
- Volume of distribution: humans 0.664L/kg; distribution half-life of 2.3 minutes
- Onset of action: Peak serum levels and initial effect seen within 2 minutes of IV administration; peak effect within 15 minutes (early studies suggested quicker peak effect).
- Metabolism:
- Though the half-life measured in the serum is 16-23 minutes, the observed half-life of plasma cholinesterase inhibition is 83-100 minutes with full recovery seen within 3 hours of cessation of infusion
- Suspected that 90% of physostigmine is metabolized by the liver within 2 minutes. The rest is metabolized locally by cholinesterase. Elimination half-life 16-23 minutes
- Indications:
- Peripheral or central anticholinergic manifestations
- Peripheral: dry mucosa, dry skin, flushed face, mydriasis, hyperthermia, decreased bowel sounds, urinary retention, tachycardia
- Central: agitation, delirium, hallucinations, seizures, coma
- Peripheral or central anticholinergic manifestations
- Dosing: 1-2mg (0.02mg/kg, max 0.5mg in children) infused over 5-10 minutes, can redose in ~15 minutes if no effect, redose in ~1 hour if initial effect that wanes
- Comes in 2mL, 1mg/mL ampules
- Case reports of infusion after initial doses lost effect (below)
- Major interactions
- Suspected interactions like RAD, intestinal/bladder obstruction
- Potentiation of paralysis with succinylcholine administration, potential inhibition/reversal of paralysis with non-depolarizing paralytic administration
- Physostigmine salicylate injection contains sodium metabisulfite; can cause anaphylactoid reactions in patients with sulfa allergies
- Management
- Before use, want to obtain ECG for potential QRS or QTc changes, (QRS < 100msec, PR < 200msec)
- Continue cardiac monitoring with pulse oximetry
- Use as an antidote
- Once was commonly used as an antidote in a wide range of anticholinergic poisonings
- However, use declined after case reports were published linking physostigmine use in TCA overdose to asystole (patients in cited literature had prolonged QRS intervals)
- More recent reviews have found little evidence that TCA ingestion or ECG changes should be used as a contraindication to physostigmine use for anticholinergic syndromes
- Cited issues seem to be speed of physostigmine infusion
- Many papers that support use as a bolus (dosing as above)
- Shown to be superior to benzodiazepines in controlling anticholinergic agitation and delirium
- Improved efficacy, decreased rates of intubation
- Has been given as a continuous infusion for persistent anticholinergic symptoms in overdose
- Clinical toxicity
- Cholinergic crisis: sweating, salivation, vomiting, diarrhea, urinary incontinence, bronchorrhea, bradycardia, hypotension, weakness, paralysis
- Potential to cause seizure
- Recommended to have atropine at the bedside of patients receiving physostigmine in the instance of overshooting the therapeutic target (especially with infusions)
References
Arens, AM et al. Safety and effectiveness of physostigmine: a 10-year retrospective review. Clin Toxicol (Phila). 2017 Jul 13:1-7.
Beaver KM, Gavin TJ. Treatment of acute anticholinergic poisoning with physostigmine. Am J Emerg Med. 1998 Sep; 16(5):505-7.
Buck ML and Reed MD. Use of nondepolarizing neuromuscular blocking agents in mechanically ventilated patients. J Clin Pharm. 1991 Jan;10(1):32-48.
Burns MJ, Linden CH, Graudins A, Brown RM, Fletcher KE. A comparison of physostigmine and benzodiazepines for the treatment of anticholinergic poisoning. Ann Emerg Med. 2000 Apr; 35(4):374-81.
Dawson, Andrew H., and Nicholas A. Buckley. Pharmacological Management of Anticholinergic Delirium ‐ Theory, Evidence and Practice. British Journal of Clinical Pharmacology 81.3 (2016): 516–524. PMC. Web. 18 Sept. 2017.
Hail SL, Obafemi A, Kleinschmidt KC. Successful management of olanzapine-induced anticholinergic agitation and delirium with a continuous intravenous infusion of physostigmine in a pediatric patient. Clin Toxicol (Phila). 2013 Mar; 51(3):162-6.Knapp S, Wardlow ML, Albert K et al.: Correlation between plasma physostigmine concentrations and percentage of acetylcholinesterase inhibition over time after controlled release of physostigmine in volunteer subjects. Drug Metab Dispos.1991;19:400–404.Pentel, P and Peterson, CD. Asystole complicating physostigmine treatment of tricyclic antidepressant overdose. Ann Emerg Med. 1980 Nov;9(11):588-90.
Rosenbaum, Christopher, and Steven B. Bird. “Timing and Frequency of Physostigmine Redosing for Antimuscarinic Toxicity.” Journal of Medical Toxicology 6.4 (2010): 386–392. PMC. Web. 18 Sept. 2017.
Phillips, Michelle A. et al. Use of a Physostigmine Continuous Infusion for the Treatment of Severe and Recurrent Antimuscarinic Toxicity in a Mixed Drug Overdose. Journal of Medical Toxicology 10.2 (2014): 205–209. PMC. Web. 18 Sept. 2017.
Schneir AB, Offerman SR, Ly BT, Davis JM, Baldwin RT, Williams SR, Clark RF. Complications of diagnostic physostigmine administration to emergency department patients. Ann Emerg Med 2003; 42: 14–9.
Suchard, JR. Assessing physostigmine's contraindication in cyclic antidepressant ingestions. J Emerg Med. 2003 Aug;25(2):185-91.
Triggle, DJ. Mitchell, JM, and Filler, R. The pharmacology or physostigmine. CNS Drug Reviews, Vol. 4, No. 2, 1998. 87-136.
Watkins JW, Schwarz ES, Arroyo-Plasencia AM, Mullins ME. The Use of Physostigmine by Toxicologists in Anticholinergic Toxicity. J Med Toxicol. 2015 Jun; 11(2):179-84.
- Introduction
- Withdrawal states can have a wide range of cardiovascular and neurological signs and symptoms
- While neurological findings such as agitation, seizures, or lethargy are often the predominant focus in management, cardiovascular changes can have significant implications on a patient’s clinical course
- Cardiomyopathies, specifically stress-induced cardiomyopathy, can accompany withdrawal states from multiple agents
- Pathophysiology
- Stress Induced Cardiomyopathy à Takotsubo Cardiomyopathy (TTC)
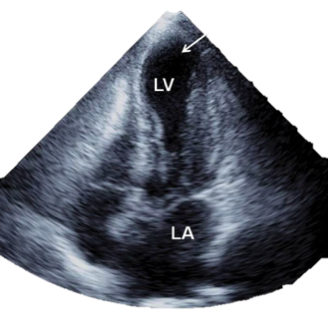
- Transient LV dysfunction due to akinesia of midapical segments without primary coronary vessel pathology
- Catecholamine toxicity leading to vasospasm of distal coronary arteries
- Supraphysiologic levels of epi change function of myocyte beta receptors
- Intracardiac gradient secondary to basal hypercontractility with LVOT obstruction causing apical ischemia/wall stress
- Stress Induced Cardiomyopathy à Takotsubo Cardiomyopathy (TTC)
References:
Stout BJ, Hoshide R, Vincent DS. Takotsubo Cardiomyopathy in the Setting of Acute Alcohol Withdrawal. Hawai’i Journal of Medicine & Public Health. 2012;71(7):193-194.
Peng TJ, Patchett ND, Bernard SA. Takotsubo Cardiomyopathy and Catatonia in the Setting of Benzodiazepine Withdrawal. Case Reports in Cardiology. 2016;2016:8153487. doi:10.1155/2016/8153487.
Spadotto V, Zorzi A, ElMaghawry M, Meggiolaro M, Pittoni GM. Heart failure due to “stress cardiomyopathy”: a severe manifestation of the opioid withdrawal syndrome. European Heart Journal Acute Cardiovascular Care. 2013;2(1):84-87. doi:10.1177/2048872612474923.
Authored by: Russell Trigonis, MD
- Offending Agents
- EtOH Withdrawal
- Most common etiology of withdrawal induced cardiomyopathy
- Chronic EtOH use alters neurotransmitter and receptor biology
- Increasing insensitivity to GABA (tolerance) with a secondary increasing of the number of glutamate receptors to allow normal state of arousal in the setting of increased inhibitory tone.
- Sudden withdrawal of EtOH decreases inhibitory tone resulting in unopposed excitatory signaling from glutamate pathways
- Peripherally presents as tremulousness and autonomic/sympathetic hyperactivity
- Benzodiazepine withdrawal
- TTC seen in few case reports following acute benzodiazepine withdrawal
- Presumed similar mechanism to EtOH
- Opioid withdrawal
- Case reports after long acting opioid methadone
- Sympathetic surge resulting in echocardiographic findings of TTC
- Methamphetamine and cocaine cardiomyopathy
- Seen during acute intoxication rather than withdrawal period
- Adrenergic surge can cause TTC or can exacerbate underlying vascular disease
- EtOH Withdrawal
- Evaluation & Treatment
- Patient may present with chest pain, shortness of breath, or other findings suggestive of LV failure
- EKG can show nonspecific findings or anterior ST elevations with minor enzyme elevations
- If there is concern for ACS PCI if available
- If no critical coronary disease, ventriculogram may show characteristic shape
- Echocardiogram with hyperactive basal segments and akinetic apex
- Supportive Care
- Ionotropic support if needed
- Anticoagulation
- Fluid balance management
- Benzodiazepines, alpha-2 agents as tolerated
- Symptoms often resolve spontaneously in 1-4 weeks
References:
Stout BJ, Hoshide R, Vincent DS. Takotsubo Cardiomyopathy in the Setting of Acute Alcohol Withdrawal. Hawai’i Journal of Medicine & Public Health. 2012;71(7):193-194.
Peng TJ, Patchett ND, Bernard SA. Takotsubo Cardiomyopathy and Catatonia in the Setting of Benzodiazepine Withdrawal. Case Reports in Cardiology. 2016;2016:8153487. doi:10.1155/2016/8153487.
Spadotto V, Zorzi A, ElMaghawry M, Meggiolaro M, Pittoni GM. Heart failure due to “stress cardiomyopathy”: a severe manifestation of the opioid withdrawal syndrome. European Heart Journal Acute Cardiovascular Care. 2013;2(1):84-87. doi:10.1177/2048872612474923.
Authored by: Russell Trigonis, MD
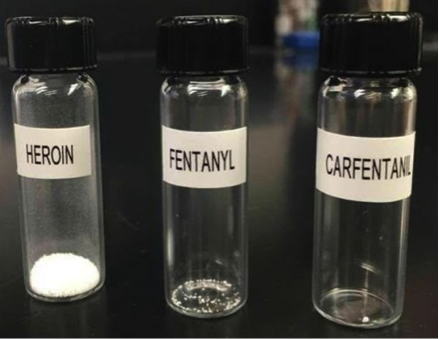
Introduction
- One of the most potent opioids created, known as Wildnil.
- This was originally created to sedate large mammals.
- Commonly used as positron emission tomography scan radioligand
- Carfentanil acts predominately on mu opioid receptors as a strong competitive agonist.
- Opiate receptors are G-protein receptors in which binding of the opiate stimulates GTP -> GDP. This decreases the intracellular cAMP by inhibiting adenylate cyclase. This hyperpolarizes the cell and reduces neurotransmitter release.
- Biological half-life 7.7 hours
- Potency 10,000 times of morphine and 100 times of fentanyl.
- Formulation: 10ml vial at 3mg/mL
- 0.005-0.02 mg/kg given to animals for sedation
Clinical Toxicity
- Altered level of consciousness -> Coma
- Respiratory depression
- Miosis
- Moscow theater hostage crisis
- Russians responded by pumping “undisclosed chemical agent” into ventilation system
- Some report naloxone was used as an antidote
- Carfentanil was identified on the clothing of some victims
- Will not be positive on routine opioid drug screen
- Felt not to cross react with fentanyl immunoassays
- Dedicated gas chromatopgraphy mass/spectrometry has been able to identify the drug as cause of death in certain case reports
Treatment/Management
- Naloxone
- Mu opioid receptor inverse agonist
- IV, IM, SubQ (onset of action 2-5 mins), Intranasal (onset of action 3-5 mins)
- Biological half life elimination: Intranasal ~2 hours, IM, IV, SubQ 0.5-1.5 hours
- Duration = 30-120 mins (IV shorter duration than IM)
- Adult dosing 0.4-4mg, child dosing 0.1 mg/kg/dose, re-dosing every 2-3 minutes
- Animal studies suggest dosing adequate response to proper dosing of naloxone to carfentanil ingestion
- Consideration of naloxone gtt especially in highly potent opioids such as carfentanil
- Can start gtt at X mg / hour that were needed to reach GCS 15
- Respiratory and hemodynamic support
- Intubation
- Vasopressors
- Observation Period
- 2-4 hours
- Looks like concrete mixing powder -> either chunky rock-like material or grey fine powder
- Combination drug of highly potent opioids including different mixtures of heroin, fentanyl, carfentanil, and U-47700
- Can be injected, inhaled, ingested, or absorbed through mucous membranes
- Touching the powder does not result in direct intoxication
- Use routine universal precautions
- Take caution if there are any breaks in skin

References1–7
1. Milone MC. Laboratory testing for prescription opioids. J Med Toxicol. 2012;8(4):4086. doi:10.1007/s13181-012-0274-7.
2. Moresco A, Larsen RS, Sleeman JM, Wild MA, Gaynor JS. USE OF NALOXONE TO REVERSE CARFENTANIL CITRATE-INDUCED HYPOXEMIA A CARDIOPULMONARY DEPRESSION IN ROCKY MOUNTAIN WAPITI (CERVUS ELAPHUS NELSONI). J Zoo Wildl Med. 2001;32(1):81-89. doi:10.1638/1042-7260(2001)032[0081:UONTRC]2.0.CO;2.
3. Klebacher R, Harris MI, Ariyaprakai N, et al. Incidence of Naloxone Redosing in the Age of the New Opioid Epidemic. Prehospital Emerg Care. 2017:1-6. doi:10.1080/10903127.2017.1335818.
4. Swanson DM, Hair LS, Strauch Rivers SR, et al. Fatalities Involving Carfentanil and Furanyl Fentanyl: Two Case Reports. J Anal Toxicol. 2017:1-5. doi:10.1093/jat/bkx037.
5. Pathan H, Williams J. Basic opioid pharmacology: an update. Br J pain. 2012;6(1):11-6. doi:10.1177/2049463712438493.
6. CARFENTANIL | C24H30N2O3 - PubChem. Available at: https://pubchem.ncbi.nlm.nih.gov/compound/carfentanil#section=Top. Accessed August 15, 2017.
7. Feasel MG, Wohlfarth A, Nilles JM, Pang S, Kristovich RL, Huestis MA. Metabolism of Carfentanil, an Ultra-Potent Opioid, in Human Liver Microsomes and Human Hepatocytes by High-Resolution Mass Spectrometry. AAPS J. 2016;18(6):1489-1499. doi:10.1208/s12248-016-9963-5.
Authored by: Katie Lupez, MD
Introduction
-Etomidate is an intravenous nonbarbiturate hypnotic
-Developed in the 1970s, found to be an effective hypnotic [1]
-Used as anesthesia induction agent and for first decade, used as sedative infusion
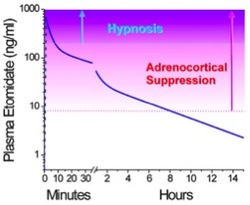
-Discovered to cause adrenal suppression and increased mortality in some critically ill patients
-Now predominately used as sedative medication in rapid sequence intubation (RSI)
Structure
-Etomidate is an intravenous nonbarbiturate hypnotic
-Developed in the 1970s, found to be an effective hypnotic [1]
-Used as anesthesia induction agent and for first decade, used as sedative infusion
-Discovered to cause adrenal suppression and increased mortality in some critically ill patients
-Now predominately used as sedative medication in rapid sequence intubation (RSI)
Structure
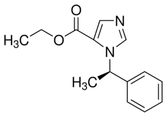
- Available as 2mg/mL solution in 35% propylene glycol solution
- Available in lipid solution in Europe, reportedly less pain on infusion
- Sedative bolus at 0.2-0.4mg/kg, general anesthesia with continuous infusion of 30-100ug/kg/min
Pharmacology/Pharmacokinetics [1]
- pKa of 4.2 and is hydrophobic at physiologic pH
- Formulated in 35% propylene glycol to increase solubility
- 75% protein bound with large volume of distribution 74.9 L/kg due to high fat solubility
- Three compartment model of pharmacokinetics for single bolus of etomidate
- Available in lipid solution in Europe, reportedly less pain on infusion
- Sedative bolus at 0.2-0.4mg/kg, general anesthesia with continuous infusion of 30-100ug/kg/min
Pharmacology/Pharmacokinetics [1]
- pKa of 4.2 and is hydrophobic at physiologic pH
- Formulated in 35% propylene glycol to increase solubility
- 75% protein bound with large volume of distribution 74.9 L/kg due to high fat solubility
- Three compartment model of pharmacokinetics for single bolus of etomidate
Compartment 1: rapid distribution into highly perfused tissue
Compartment 2: redistribution into peripheral tissues (muscles)
Compartment 3: terminal metabolism
Compartment 2: redistribution into peripheral tissues (muscles)
Compartment 3: terminal metabolism
- Onset of action in <1min, duration is approximately 5 min
- Metabolism dependent on hepatic esterase activity, which hydrolyzes to carboxylic acid and an ethanol leaving group
- Carboxylate metabolite mostly excreted in urine
- Metabolic t1/2 ranges from 2-5 hours
- Elderly or ill patients require lower etomidate doses due to reduced protein binding and reduced clearance
Mechanism of Action:
- Non barbiturate hypnotic active at the GABAA receptor, specifically the β2 and β3
- Etomidate positively modulates GABAA activation by agonists
- Slow postsynaptic current decay, prolonging postsynaptic inhibition
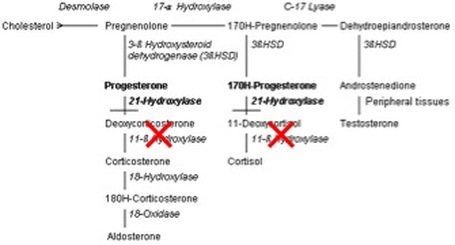
- Blocks 11β-hydroxylase in the steroidogenesis pathway [2]
- Nitrogen atom of the imidazole ring interacts with the active binding site of the enzyme
- Metabolism dependent on hepatic esterase activity, which hydrolyzes to carboxylic acid and an ethanol leaving group
- Carboxylate metabolite mostly excreted in urine
- Metabolic t1/2 ranges from 2-5 hours
- Elderly or ill patients require lower etomidate doses due to reduced protein binding and reduced clearance
Mechanism of Action:
- Non barbiturate hypnotic active at the GABAA receptor, specifically the β2 and β3
- Etomidate positively modulates GABAA activation by agonists
- Slow postsynaptic current decay, prolonging postsynaptic inhibition
- Blocks 11β-hydroxylase in the steroidogenesis pathway [2]
- Nitrogen atom of the imidazole ring interacts with the active binding site of the enzyme
Toxicity
- Propylene glycol diluent is implicated in development of hyperosmolar metabolic acidosis when used in prolonged infusions
- Cardiovascular side effects include hypotension and tachycardia, less significant than most other sedative agents
- Both proconvulsant and anticonvulsant properties
- Myoclonus- may be caused by etomidate interaction with glycine receptor at the spinal cord level
- Adrenocortical suppression- etomidate blocks of 11β-hydroxylase leading to depressed adrenal production of cortisol and aldosterone
- Pain on infusion
- Myoclonus
- Postoperative nausea and vomiting (40%)- few studies have compared etomidate vs. other induction agents. One study has shown this to be comparable to barbituates and higher than propofol [1]
- Adrenocortical inhibition- can manifest as hypotension refractory to fluids and vasopressors
Management
- Pain on infusion- consider pretreatment with 3mL 1% lidocaine
- Nausea and vomiting- symptomatic treatment
- Myoclonus- opioid (fentanyl derivatives, dezocine) [7] , magnesium [8] , ketamine [9] pretreatment
- Adrenal suppression- should we treat with corticosteroids?
Future Directions
Novel etomidate agents-
Carboetomidate- contains pyrrole instead of imidazole, making binding 11β-hydroxylase less effective and thus reducing adrenal suppression [12]
MOC-etomidate- Alteration made to ester moiety that is then rapidly metabolized, producing less profound and shorter-lasting adrenal suppression [12]
- Propylene glycol diluent is implicated in development of hyperosmolar metabolic acidosis when used in prolonged infusions
- Cardiovascular side effects include hypotension and tachycardia, less significant than most other sedative agents
- Both proconvulsant and anticonvulsant properties
- Myoclonus- may be caused by etomidate interaction with glycine receptor at the spinal cord level
- Adrenocortical suppression- etomidate blocks of 11β-hydroxylase leading to depressed adrenal production of cortisol and aldosterone
- This has been found in both single dose administrations of etomidate[3] and in prolonged infusions of etomidate[1]
- Adrenal suppression lasting >24hrs following infusion, 6-8hrs following bolus
- Increased mortality
- Related to prolonged etomidate infusions
- 1983 study reported retrospective data that showed increased mortality among ICU patients receving prolonged etomidate infusions compared to those receiving benzodiazepine infusions (69% vs. 25%) [4]
- Several studies have cited increased mortality in critically ill patients following a single induction dose of etomidate, however several recent studies refute these conclusions:
- Etomidate vs. ketamine for RSI in acutely ill patients (KETASED) trial, Lancet 2009
- Study of 655 patients requiring emergent RSI in prehospital, ED, or ICU
- No statistically significant difference was seen in sepsis-related organ failure, mortality rates, or intubating conditions between the 2 groups. However, there was a higher incidence of adrenal insufficiency in the etomidate group (defined as serum cortisol <10ug/dL or difference of <9ug/dL sixty min after ACTH stimulation test) – 86% in those with etomidate vs. 56% in those without etomidate use (p<0.0001) [5]
- Most recent Cochrane systematic review of evidence suggests that “no strong evidence exists that etomidate increases mortality in critically ill patients when compared to other bolus dose induction agents” [6]
- Pain on infusion
- Myoclonus
- Postoperative nausea and vomiting (40%)- few studies have compared etomidate vs. other induction agents. One study has shown this to be comparable to barbituates and higher than propofol [1]
- Adrenocortical inhibition- can manifest as hypotension refractory to fluids and vasopressors
Management
- Pain on infusion- consider pretreatment with 3mL 1% lidocaine
- Nausea and vomiting- symptomatic treatment
- Myoclonus- opioid (fentanyl derivatives, dezocine) [7] , magnesium [8] , ketamine [9] pretreatment
- Adrenal suppression- should we treat with corticosteroids?
- Corticosteroid Therapy of Septic Shock (CORTICUS) trial, NEJM 200810
- Study of 499 critically ill patients in 52 ICUs, 9 countries
- Hydrocortisone shown to hasten recovery of blood pressure in septic shock but did not have an impact on mortality
- Data revealed increased rate of death at 28 days among patients who received etomidate before randomization (40-45.1% in placebo/hydrocortisone groups respectively) vs. those who had not received etomidate before randomization (29.6-31.5% in placebo/hydrocortisone groups respectively; P= 0.03)
- The data in this study were not evaluated in the Cochrane review due to observational nature of etomidate exposure and there was no causation determined. The more recent KETASED trial has suggested no change in mortality data.
- 2012 Surviving sepsis guidelines- Recommend against using corticosteroids if hypotension is responsive to fluids and vasopressors (level 2C). When significant hemodynamic instability remains following fluids and vasopressors, corticosteroids are recommend at an IV dose of 200 mg hydrocortisone every 24 hours [11]
Future Directions
Novel etomidate agents-
Carboetomidate- contains pyrrole instead of imidazole, making binding 11β-hydroxylase less effective and thus reducing adrenal suppression [12]
MOC-etomidate- Alteration made to ester moiety that is then rapidly metabolized, producing less profound and shorter-lasting adrenal suppression [12]

Use in severe Cushing’s syndrome- several case studies outlining the use of etomidate infusions as low as 2.5mg/hr resulting in clinical improvement in hypercortisolism without causing sedative effects [13]
References
1. Forman, S. Clinical and Molecular Pharmacology of Etomidate. Anesthesiology 2011; 114(3): 695-707.
2. de Jong FH, Mallios C, Jansen C, Scheck PA, Lamberts SW. Etomidate suppresses adrenocortical function by inhibition of 11 beta-hydroxylation. J Clin Endocrinol Metab 1984; 59: 1143–47.
3. Hildreth AN, Mejia VA, Maxwell RA, Smith PW, Dart BW, Barker DE. Adrenal suppression following a single dose of etomidate for rapid sequence induction: a prospective randomized study. J Trauma 2008; 65: 573–79.
4. Ledingham IM, Watt I. Influence of sedation on mortality in critically ill multiple trauma patients. Lancet 1983; 321: 1270.
5. P. Jabre, X. Combes, F. Lapostolle, M. Dhaouadi, A. Ricard-Hibon, B. Vivien, Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial, Lancet, Vol. 374, 2009, 293-300
6. Bruder EA, Ball IM, Ridi S, Pickett W, Hohl C. Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients. Cochrane Database of Systematic Reviews 2015, Issue 1
7. Li, Z., He, L., Diny, Y., Chen, H. Dezocine pretreatment prevents myoclonus induced by etomidate: a randomized, double-blinded controlled trial, Anesthesiology 2015. 29(1):143-145.
8. Yelken, B., Un, B., Ceyhand, D. Prevention of etomidate-related myoclonus in anesthetic induction by pretreatment with magnesium. J. Res Med Sci 2011, 16(11):1490-1494.
9. Zhou, H., Wu, GN, Xu, HJ, Wu X. Low-dose Ketamine Pretreatment Reduces the Incidence and Severity of Myoclonus Induced by Etomidate: A randomized, Double-Blinded, Controlled Clinical Trial. Medicine 2016, 95(6)
10. Briegel, J. and CORTICUS study group. Hydrocortisone Therapy for Patients with Septic Shock. New Eng J Med 2008. 358(2): 111-124.
11. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Crit Care Med. 2013;41:580–637
12. Sney, J. Novel Etomidate Derivatives. Current Pharm Design 2012, 18: 6253-6256.
13. Price-Newell, J., Daniel, E. Therapy of Endocrine Disease: Steroidogenesis enzyme inhibitors in Cushing’s Syndrome. Eur J Endocrinol 2015. 172: 263-280.
Other sources used include Goldfrank’s 10th edition, Haddad’s 3rd edition, and The Poison Review (www.thepoisonreview.com)
Authored by: Dr. Cate Lounsbury, MD
1. Forman, S. Clinical and Molecular Pharmacology of Etomidate. Anesthesiology 2011; 114(3): 695-707.
2. de Jong FH, Mallios C, Jansen C, Scheck PA, Lamberts SW. Etomidate suppresses adrenocortical function by inhibition of 11 beta-hydroxylation. J Clin Endocrinol Metab 1984; 59: 1143–47.
3. Hildreth AN, Mejia VA, Maxwell RA, Smith PW, Dart BW, Barker DE. Adrenal suppression following a single dose of etomidate for rapid sequence induction: a prospective randomized study. J Trauma 2008; 65: 573–79.
4. Ledingham IM, Watt I. Influence of sedation on mortality in critically ill multiple trauma patients. Lancet 1983; 321: 1270.
5. P. Jabre, X. Combes, F. Lapostolle, M. Dhaouadi, A. Ricard-Hibon, B. Vivien, Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial, Lancet, Vol. 374, 2009, 293-300
6. Bruder EA, Ball IM, Ridi S, Pickett W, Hohl C. Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients. Cochrane Database of Systematic Reviews 2015, Issue 1
7. Li, Z., He, L., Diny, Y., Chen, H. Dezocine pretreatment prevents myoclonus induced by etomidate: a randomized, double-blinded controlled trial, Anesthesiology 2015. 29(1):143-145.
8. Yelken, B., Un, B., Ceyhand, D. Prevention of etomidate-related myoclonus in anesthetic induction by pretreatment with magnesium. J. Res Med Sci 2011, 16(11):1490-1494.
9. Zhou, H., Wu, GN, Xu, HJ, Wu X. Low-dose Ketamine Pretreatment Reduces the Incidence and Severity of Myoclonus Induced by Etomidate: A randomized, Double-Blinded, Controlled Clinical Trial. Medicine 2016, 95(6)
10. Briegel, J. and CORTICUS study group. Hydrocortisone Therapy for Patients with Septic Shock. New Eng J Med 2008. 358(2): 111-124.
11. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Crit Care Med. 2013;41:580–637
12. Sney, J. Novel Etomidate Derivatives. Current Pharm Design 2012, 18: 6253-6256.
13. Price-Newell, J., Daniel, E. Therapy of Endocrine Disease: Steroidogenesis enzyme inhibitors in Cushing’s Syndrome. Eur J Endocrinol 2015. 172: 263-280.
Other sources used include Goldfrank’s 10th edition, Haddad’s 3rd edition, and The Poison Review (www.thepoisonreview.com)
Authored by: Dr. Cate Lounsbury, MD
Toxicology Blog

Author
EM Rotators on Toxicology
Selected by Feedspot as one of the Top 20 Toxicology Blogs on the web
Archives
March 2018
November 2017
October 2017
August 2017
April 2016
November 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
Categories
All
Bath Salts
Domoic Acid
Etomidate
Herbals
Intralipid Therapy
Mercury
Overdose
Precedex
Propofol
SSRI
Disclaimer: All images included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
 RSS Feed
RSS Feed
