|
Authored by Dr. Enola Okonkwo Introduction Artemether Lumefantrine is an oral medication which is used in treatment of chloroquine resistant uncomplicated malaria. Artemether Lumefantrine falls within the drug class of Artemisinin-based combination therapies which have been found to be highly effective in treating malaria and are substantially less toxic than quinoline antimalarials. Artemisins are derived from a Chinese medicinal herb which comes from the sweet wormwood plant (1). Artemether Lumefantrine, known by the brand name Coartem, is the most widely used artemisinin based combination therapy used in Africa and is one of three medications recommended by the CDC as first line oral treatment for uncomplicated falciparum malaria within the United States (2). Structure 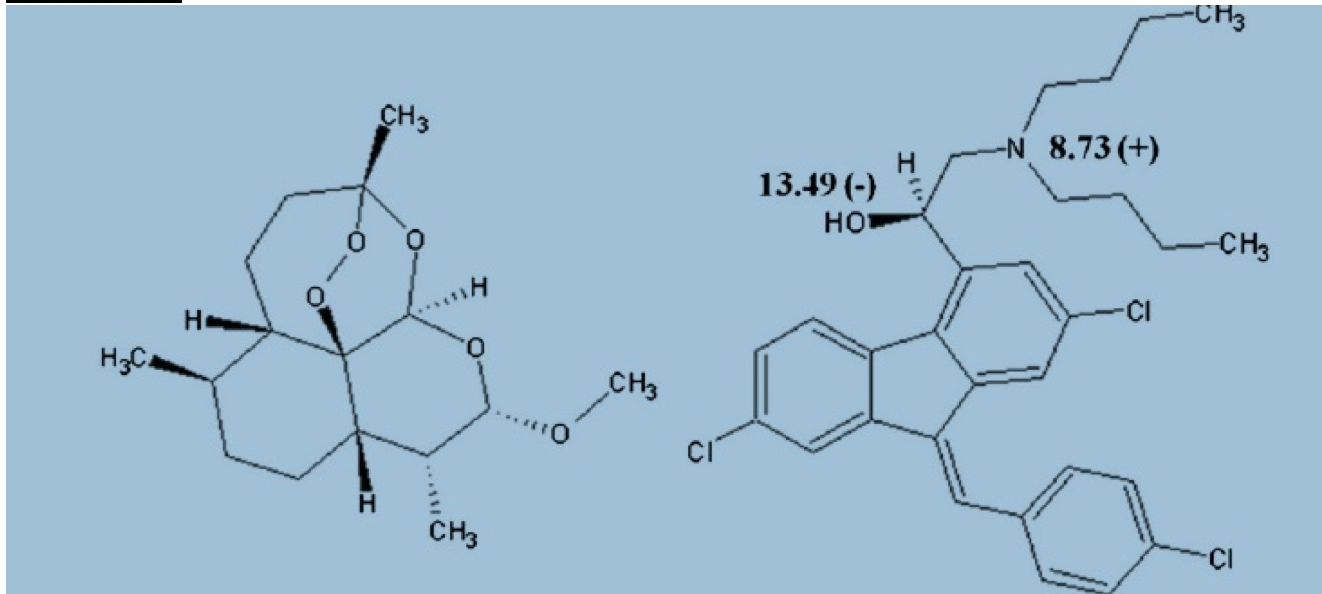 1 tablet = 20mg artemether and 120 mg lumefantrine.
Dosing is weight based. For patients > 35 kg they are taking 4 tablets per dose twice daily for 3 days. Pharmacology/Pharmacokinetics: Absorption/Distribution/Metabolism/Excretion Artemeter is rapidly absorbed. Peak plasma level of artemeter is approximately 2 hours. The half-life after ingestion is 2 hours (4-5). 95% of artemether is protein bound but quickly undergoes metabolism to dihydroartemisin which is approximately 50% protein bound. Half life of dihydroartemisin is also around 2 hours (5). Bioavailability increased 2-3 fold when consumed with food (4). Lumefantrine – Initial absorption at approximately 2 hours. Peak plasma level approximately 6-8 hours. Half life is 4-5 days. It is highly protein bound and has a large volume of distribution. High fat meals significantly increase absorption 16 fold (4). Significant Drug/Drug interactions Numerous theoretic drug interactions have been reported. However, there is scant data available reporting clinical effects of drug interactions. -May enhance QTc prolonging effects -May enhance toxic effects of other antimalarial or HIV medications -May increase serum concentration of antipsychotics -May decrease serum concentration of estrogen related contraceptives -May decrease serum concentration of CYP3A4 Substrates Metabolic Pathways and active metabolites Arthemeter is metabolized by the liver to the active metabolite dihydroartemisinin primarily by CYP3A4/5. Lumefantrine is metabolized by the liver to desbutyl-lumefantrine by CYP3A4. Studies suggest that artemisins inhibit the sarco/endoplasmic reticulum Ca ATPases of the malaria parasite causing rapid reduction in the parasite (6-7). The mechanism of lumefantrine is unknown but both agents inhibit nucleic acid and protein synthesis. Artemether rapidly kills the majority of the parasite and lumefantrine goes on to kill the residual remaining parasite (4-5). Mechanism of Toxicity Artemether Lumefantrine has been extensively used for the treatment of malaria and appears to have an excellent safety profile. There are no reported overdoses or intentional ingestions. There has been no evidence of significant systemic or local toxicity reported in any large human study (1, 20-21). However, there is animal data and a few small human studies and case reports which suggest neurotoxicity and QT prolongation are possible toxic effects of artimisinins (14). Neurotoxicity was especially common in animal studies both clinically and histologically (8-10, 14). In vitro studies have postulated that neurotoxicity results secondary to ATP depletion of neurons and free radical generation created by the breakdown of artemisins (Schmuck 2002, Smith 1998) . Toover et. el wrote a review article cautioning that neurotoxic effects may also occur in humans more frequently than previously thought, though many critics viewed their review as bias (8, 13). There are a small number of case reports within humans suggesting that artemisins contributed to neurologic symptoms such as anxiety, tremor, and ataxia (8, 15-16). A small study looking at construction workers treated with arthemeter suggested that individuals had hearing loss following the administration of artemether (17). Obviously, this study is limited by a serious potential confounder and attempts to reproduce these results have failed (18). One case report of delayed hemolytic anemia, not thought to be related to malaria was reported (19). Clinical Toxicity Given patients taking artemether lumefantrine have malaria, it is difficult to distinguish between symptoms caused by the disease state of malaria versus symptoms which may be attributed to medication toxicity. Clinical toxicity appears to be very rare or possibly underreported. A large review of 188 studies including over 9,000 patients found no serious clinical toxicity (21). This review article used methodology similar to Cochrane review and reported transient neutropenia in 1.3%, reticulocytopenia (0.6%), elevated liver enzymes (0.9%), and transient bradycardia and prolonged QT (1.1%). The most common side effects reported were gastrointestinal. The authors conclude that Artemether Lumefantrine is a safe and efficacious drug. Common adverse events (4, 20-21) Abdominal pain Anorexia Vomiting Diarrhea Headache dizziness. Pruritis and Rash < 2% Laboratories No specific toxicology labs are available Management of Toxicity No accepted recommendations regarding toxicity given the scarcity of data suggesting toxicity. Below are general recommendations based off of literature review: Avoid concurrent use of additional antimalarial medications Use caution administering additional drugs which can prolong QT Use caution in hypokalemia and replete electrolytes as needed Use caution in patients with prolonged QT Obtain EKG as screening for arrhythmia References: 1. Hien, T. T., White, N. J., & White. (1993). Qinghaosu. The Lancet, 341(8845), 603–608. https://doi.org/10.1016/0140-6736(93)90362-K 2. Center for Disease Control. (2009). Guidelines for treatment of malaria in the United States. Treatment Table Update, May, (770), 855–857. Retrieved from http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Guidelines+for+Treatment+of+Malaria+in+the+United+States#1 3. Amin, N. C., Fabre, H., Blanchin, M.-D., Montels, J., & Aké, M. (2013). Determination of artemether and lumefantrine in anti-malarial fixed-dose combination tablets by microemulsion electrokinetic chromatography with short-end injection procedure. Malaria Journal, 12, 202. https://doi.org/10.1186/1475-2875-12-202 4. Waning, B., & Montange, M. (2015). Access Pharmacy. Retrieved from http://accesspharmacy.mhmedical.com/content.aspx?bookid=438§ionid=40428529 5. White, N. J., Van Vugt, M., & Ezzet, F. (1999). Clinical pharmacokinetics and pharmacodynamics of artemether-lumefantrine. Clinical Pharmacokinetics. Adis International Ltd. https://doi.org/10.2165/00003088-199937020-00002 6. Krishna, S., Pulcini, S., Moore, C. M., Teo, B. H. Y., & Staines, H. M. (2014, January). Pumped up: Reflections on PfATP6 as the target for artemisinins. Trends in Pharmacological Sciences. https://doi.org/10.1016/j.tips.2013.10.007 7. Eckstein-Ludwig, U., Webb, R. J., Van Goethem, I. D. A., East, J. M., Lee, A. G., Kimura, M., … Krishna, S. (2003). Artemisinins target the SERCA of Plasmodium falciparum. Nature, 424(6951), 957–961. https://doi.org/10.1038/nature01813 8. Toovey, S. (2006, October 10). Are currently deployed artemisinins neurotoxic? Toxicology Letters. https://doi.org/10.1016/j.toxlet.2006.06.001 9. Genovese, R. F., Newman, D. B., Li, Q., Peggins, J. O., & Brewer, T. G. (1998). Dose-dependent brainstem neuropathology following repeated arteether administration in rats. Brain Research Bulletin, 45(2), 199–202. https://doi.org/10.1016/S0361-9230(97)00339-0 10. Petras, J. M., Young, G. D., Bauman, R. A., Kyle, D. E., Gettayacamin, M., Webster, H. K., … Brewer, T. G. (2000). Arteether-induced brain injury in Macaca mulatta. I. The precerebellar nuclei: The lateral reticular nuclei, paramedian reticular nuclei, and perihypoglossal nuclei. Anatomy and Embryology, 201(5), 383–397. https://doi.org/10.1007/s004290050326 11. Schmuck, G., Roehrdanz, E., Haynes, R. K., & Kahl, R. (2002). Neurotoxic mode of action of artemisinin. Antimicrobial Agents and Chemotherapy, 46(3), 821–827. https://doi.org/10.1128/AAC.46.3.821-827.2002 12. Smith, S. L., Maggs, J. L., Edwards, G., Ward, S. A., Park, B. K., & McLean, W. G. (1998). The role of iron in neurotoxicity: a study of novel antimalarial drugs. Neurotoxicology, 19(4–5), 557–559. 13. Toovey, S. (2006, October 10). Are currently deployed artemisinins neurotoxic? Toxicology Letters. https://doi.org/10.1016/j.toxlet.2006.06.001 14. Brewer, T. G., Peggins, J. O., Grate, S. J., Petras, J. M., Levine, B. S., Weina, P. J., … Schuster, B. G. (1994). Neurotoxicity in animals due to arteether and artemether. Transactions of the Royal Society of Tropical Medicine and Hygiene, 88, 33–36. https://doi.org/10.1016/0035-9203(94)90469-3 15. Miller, L. G., & Panosian, C. B. (1997). Ataxia and slurred speech after artesunate treatment for falciparum malaria. New England Journal of Medicine, 336(18), 1328. https://doi.org/10.1056/NEJM199705013361818 16. Franco-Paredes, C., Dismukes, R., Nicolls, D., & Kozarsky, P. E. . (2005). Neurotoxicity Due to Antimalarial Therapy Associated with Misdiagnosis of Malaria. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 40(11), 1710–1711. https://doi.org/10.1086/430180 17. Toovey, S. (2006). A case-control auditory evaluation of patients treated with artemether-lumefantrine. American Journal of Tropical Medicine and Hygeine 74, 939-940. 18. Hutagalung, R., Htoo, H., Nwee, P., Arunkamomkiri, J., Zwang, J., Carrara, V. I., … Nosten, F. (2006). A case-control auditory evaluation of patients treated with artemether-lumefantrine. American Journal of Tropical Medicine and Hygiene, 74(2), 211–214. https://doi.org/74/2/211 [pii] 19. Hasegawa, C., Kudo, M., Maruyama, H., Kimura, M. (2017). Severe delayed haemolytic anaemia associated with artemether-lumefantrine treatment of malaria in a Japanese traveler. Journal of Infection and Chemotherapy. In press. https://doi.org/10.1016/j.jiac.2017.10.008 20. Alkadi, H. O. (2007, November). Antimalarial drug toxicity: A review. Chemotherapy. https://doi.org/10.1159/000109767 21. Ribeiro, I. R., & Olliaro, P. (1998). Safety of artemisinin and its derivatives. A review of published and unpublished clinical trials. Medecine Tropicale : Revue Du Corps de Sante Colonial, 58(3 Suppl), 50–53. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=10212898
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Toxicology Blog
AuthorEM Rotators on Toxicology Selected by Feedspot as one of the Top 20 Toxicology Blogs on the web
Archives
March 2018
Categories
All
Disclaimer: All images included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
