|
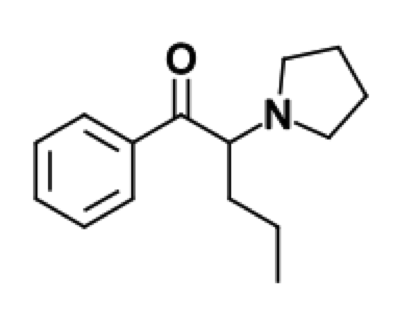
Alpha-PVP (aka “Flakka” or “Gravel”) Introduction: -Also referred to as Alpha-pyrrolidinovalerophenone, alpha-pyrrolidinopentiophenone, (RS)-1-phenyl-2-(1-pyrrolidinyl)-1-pentanone -Cathinone is a natural stimulant found in the khat plant -Synthetic cathinones, aka “Bath salts”, refer to a collective group of compounds that are highly potent stimulants and are similar to MDMA, cocaine, and methamphetamine -The most common compound found in bath salts is MDPV (3,4-methylenedioxypyrovalerone) -Alpha-PVP is not a “second generation bath salt”; it was actually first synthesized in the 1960’s -Alpha-PVP has been recently been linked to multiple reported deaths in Florida -Alpha-PVP was added to the controlled substance list in the USA in 2014 Structure: -Alpha-PVP typically comes in a crystal form -Formula: C15H21NO
Pharmacology/Pharmacokinetics:
-Alpha-PVP’s mechanism of action is believed to involve inhibition of the reuptake of norepinephrine, dopamine, and serotonin -Rat studies have showed that alpha-PVP is both an uptake blocker of norephinephrine/dopamine and stimulates dopamine release Absorption/Distribution/Metabolism/Excretion: Absorption -Can be taken orally, sublingually, injected, vaporized, or intranasal -Onset of desired effects (euphoria) in 5-30 minutes and lasts for 1-3 hours. However, the undesired side effects (including psychosis) can last days Distribution -Postmortem studies have found alpha-PVP uniformly distributed among multiple tissues (blood, brain, muscle, CSF, lung, kidney, and liver) Metabolism -Six phase I metabolites have been identified -Lactam is the major metabolite Excretion -A study of postmortem alpha-PVP levels showed the highest concentrations were found in urine and the lowest concentrations were found in the liver → suggesting the drug is excreted chiefly by the renal system Significant Drug/Drug Interactions: -Co-ingestion of alcohol, other stimulants, and other illicit drugs has been shown to enhance the effects of the drugs -A large proportion of the fatal cases of alpha-PVP have involved co-ingestions of multiples drugs and alcohol Toxicity/Mechanism of Toxicity: -LD50 has not been determined -The potency and efficacy of alpha-PVP and MDPV are very similar in rat studies -Rat studies showed increased locomotor signs with doses ranging from 1mg/kg to 30mg/kg -A few case reports of drug-related fatalities with serum alpha-PVP levels have been reported: 0.1mg/L, 0.29mg/L, 0.52mg/L, 0.901mg/L -All serum levels determined by liquid-mass-mass spectrometry method -There is a significant overlap between concentrations tolerated by individuals and those reported in drug-related fatalities → alpha-PVP concentration alone does not determine toxicity Clinical Toxicity/Presentation: -Increased dopamine causes euphoria, increased activity, and hyperstimulation -Increased norepinephrine increases heart rate and blood pressure -Increased serotonin can cause hallucinations, delirium, and paranoia -Severe agitated delirium and aggressive behavior have been reported -Life threatening severe toxicity: Serotonin syndrome, hyperthermia, hypotension, rhabdomyolysis, acute renal failure, liver failure, cardiac dysrhythmias, seizures -Chronic exposure: May lead to physical and psychological dependence with withdrawal symptoms Laboratories/Where it is made: -Mainly manufactured in China and India and then shipped to America by legal delivery companies -Unknown if manufactured in America currently Treatment/Management: -Treatment is symptomatic and supportive -Benzodiazepines for sedation/delirium/seizures/tachycardia/hypertension -IVF’s for dehydration frequently indicated -GI decontamination is not recommended. Single dose of activated charcoal may be considered for possible co-ingestion, but usually not clinically indicated. Hemodialysis is not effective for elimination. -Labs: Obtain electrolytes, renal function, hepatic enzymes, and CPK level -Serum drug levels are NOT clinically useful and NOT readily available -Obtain EKG and continuous cardiac monitoring -Frequent temperature monitoring and institute cooling measures as warranted (Hyperthermia is an indicator of severe toxicity) -Dispo: Minimal observation of 6-8 hours. If patient has persistent CNS stimulation, persistent tachycardia, seizures, or dysrhythmias →then warrants admission -Poison center should be consulted By: Dr. Patrick Jackson References:
0 Comments
|
Toxicology Blog
AuthorEM Rotators on Toxicology Selected by Feedspot as one of the Top 20 Toxicology Blogs on the web
Archives
March 2018
Categories
All
Disclaimer: All images included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
