|
Authored by Dr. Kyle Roedersheimer Introduction to ADHD
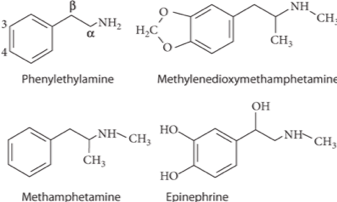
History of Amphetamines
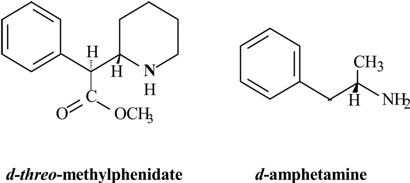
Psychostimulants
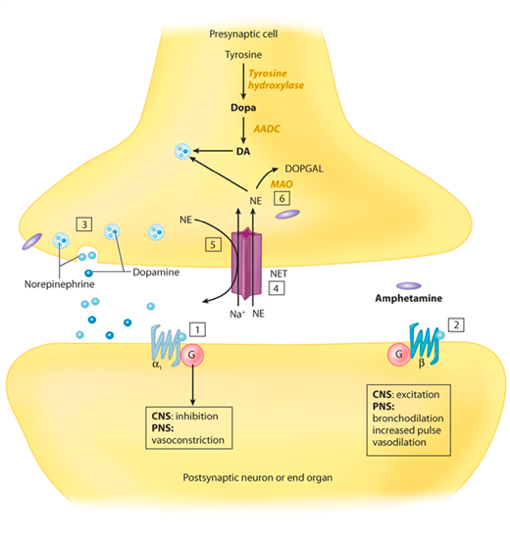
Mechanism of action
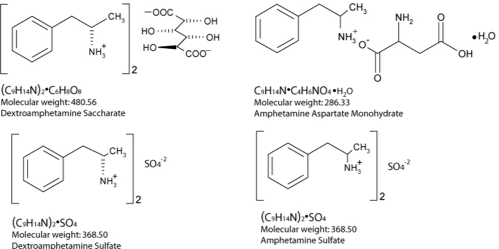
Pharmacology/Pharmacokinetics:
Therapeutic levels
Significant Drug/Drug Interactions
Metabolic Pathways and active metabolites
Diagnostic Testing and Laboratories
Treatment/Management
What is Stuttering? What causes it?
Multiple Case Reports Discussing Stuttering Associated with ADHD Medications
References
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Toxicology Blog
AuthorEM Rotators on Toxicology Selected by Feedspot as one of the Top 20 Toxicology Blogs on the web
Archives
March 2018
Categories
All
Disclaimer: All images included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
