|
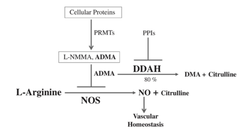
Authored By: Meredith Binford Background: Proton pump inhibitors (PPIs) inhibit H+K+ATPase proton pumps in the stomach to reduce acid excretion. Among the most frequently prescribed drugs worldwide and are generally well tolerated. Now they are available for long-term use without medical supervision. Often prescribed to circumvent GI side effects from dual antiplatelet agents used for cardiovascular disease secondary prevention. However recent observational studies have linked PPI use to increased cardiovascular risk (MI and stroke) even in patients not taking antiplatelet agents. Mechanism: -impair lysosomal acidification and enzyme activity -accelerate telomere erosion -speed endothelial aging as manifested by impaired cell perforation and angiogenesis -impair the NO synthase pathway though asymmetric dimethylarginine (ADMA)
3 recent articles investigate PPIs and risk of stroke: 1. A large retrospective study from the Taiwan National Health Insurance Database studied whether PPI use alone could be associated with first time ischemic stroke. In a propensity score matched analysis (400,000 patients) over 120 days PPI use was associated with a higher risk of hospitalization due to ischemic stroke with hazard ratio of 1.36 (95% CI 1.14-1.62, P=0.001). In subgroup analysis, the risk was more prominent in those less than 60 years of age but gender, prior MI, diabetes, hypertension, use of antiplatelet agents or NSAIDs, or types of PPI did not have an influence on the risk. In the nested case-control analysis (30,000 patients), the adjusted odds ratios for PPI use were 1.77 (95% CI 1.45-2.17, P<0.001) within 30 days and 1.65 (95% CI 1.31-2.08, P<0.001) 31 to 90 days before ischemic stroke. The proportions of H2 blocker users and non users were comparable before the event. One of the major arguments against the association is confounding by indication for PPI use as PPIs are used over H2 blockers in the presence of more severe acid related GI disorders. Other uncorrected confounders include obesity, lack of exercise, smoking, compliance with hypertension treatment, diabetes, hyperlipidemia, other medical illnesses. Also limited by 120 day follow up which may have masked confounders of PPI use. 2. Danish registry of people who underwent elective EGD (215,000 patients) was analyzed in a time varying design to asses dose response effects on hazard ratios as well as in a baseline treatment design to show impact of long term use on risks of first time stroke and MI. Current PPI exposure was associated with significantly higher rates of both ischemic stroke with hazard ratio of 1.13 (95% CI 1.08-1.19) and MI with hazard ratio of 1.31 (95% CI 1.23-1.39) after adjusting for age, sex, comorbidities and concomitant medications. High dose PPI was associated with increased rates of ischemic stroke with hazard ratio of 1.31 (95% CI 1.21-1.42) and MI with hazard ratio of 1.43 (95% CI 1.30-1.57). H2 blockers were not significantly associated with ischemic stroke or MI. Long-term PPI users had a 29% greater absolute risk of ischemic stroke and a 36% greater absolute risk of MI within six months period. One limitation is confounding that PPI identifies unhealthy individuals. When estimating impact of smoking habit, obesity, and exercise the net confounding bias was between 3.8 and 4.1% which reduced the hazard ratio to 1.08 for ischemic stroke and 1.26 for MI. Also concern of a lead in bias as subjects were likely exposed to PPI therapy before EGD. 3. Analysis from the Nurses Health Study and the Health Professionals Follow Up Study (950,000 person years) observed an association between regular PPI use and risk of ischemic stroke in age-adjusted models and multivariate models adjusting for known risk factors for ischemic stroke that was consistent with findings of prior reports. However additional adjustment for factors that may be associated with initiation and continuation of PPI therapy including history of peptic ulcer disease, GERD, GI bleeding and prior H2 blocker use substantially attenuated the association. They found that participants who were regular PPI users at baseline tended to have higher rates of chronic medical conditions including prior history of hypertension, hyperlipidemia, CAD, diabetes, as well as lower levels of physical activity expenditure. Among women, regular PPI users were more likely to have a higher BMI and a prior history of menopausal hormonal use. Association of PPI use with ischemic stroke may be due to residual confounding by factors associated with the indication for PPI use, for example metabolic syndrome. Conclusion: There is a plausible biological mechanism to explain the association of PPIs with increased cardiovascular risk. Large retrospective studies show association especially with longer use and higher dose PPI. However there is concern of confounding as may be related to more unhealthy patients using PPIs. References: Sehested, TSG et al. Long term use of proton pump inhibitors, dose-response relationship and associated risk of scheming stroke and myocardial infarction. Journal Internal Medicine 2017, doi: 10.1111/joim.12698. Nguyen LH, Lochhead P, Joshi AD, Cao Y, Ma W, Khalili H, Rimm EB, Rexrode KN< Chan AT. No significant association between proton pump inhibitor use and risk of stroke after adjustment for lifestyle factors and indication. Gastroenterology 2018, doi: 10.1053/j.gastro.2017.12.006. Wang Y-F, Chen Y-T, Luo J-C, Chen T-J, Wu J-C, Wang S- J. Proton-pump inhibitor use and the risk of first-time ischemic stroke in the general population: a nationwide population-based study. Am J Gastroenterol 2017; 112: 1– 10. Yepuri G, Sukhovershin R, Nazari-Shafti TZ, Petrascheck M, Ghebre YT, Cooke JP. Proton pump inhibitors accel- erate endothelial senescence. Circ Res 2016; 118: e36–42. Ghebremariam YT, Lependu P, Lee JC et al. Unexpected effect of proton pump inhibitors: elevation of the cardiovascular risk factor asymmetric dimethylarginine. Circulation 2013; 128: 845–53. Cooke JP. Asymmetrical dimethylarginine: the u€ber marker? Circulation 2004; 109: 1813–9.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Toxicology Blog
AuthorEM Rotators on Toxicology Selected by Feedspot as one of the Top 20 Toxicology Blogs on the web
Archives
March 2018
Categories
All
Disclaimer: All images included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
