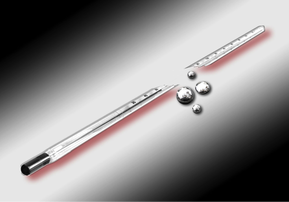
Elemental Mercury – used for home metallurgy, gold smithing, thermometers
 Guiterrez, F. Leon, L. Elemental Mercury Embolism to the Lung. N Engle J Med 2000; 342: 1791. June 15, 2000.  Inorganic Mercury
Management
Antidotes – Chelation Therapy!
Dimercaprol (BAL) – Acute elemental and inorganic mercury
References 1. Aaseth J, Skaug MA, Cao Y, Andersen O. Chelation in metal intoxication-Principles and paradigms. J Trace Elem Med Biol. 2014 2. Cao Y, Skaug MA, Andersen O, Aaseth J. Chelation therapy in intoxications with mercury, lead and copper. J Trace Elem Med Biol. 2014; 3. George GN, Prince RC, Gailer J, et al. Mercury binding to the chelation therapy agents DMSA and DMPS and the rational design of custom chelators for mercury. Chem Res Toxicol. 2004;17(8):999-1006. 4. Sue Y. Chapter 96. Mercury. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. Eds. Goldfrank’s Toxicologic Emergencies, 9e. New York, NY: McGraw-Hill 2011. 5. Guiterrez, F. Leon, L. Elemental Mercury Embolism to the Lung. N Engl J Med 2000; 342: 1791. June 15, 2000. 6. Aaseth J, Jacobsen D, Andersen O, Wickstrøm E. Treatment of mercury and lead poisonings with dimercaptosuccinic acid and sodium dimercaptopropanesulfonate. A review. Analyst. 1995;120(3):853-4. 7. Aposhian HV, Maiorino RM, Gonzalez-ramirez D, et al. Mobilization of heavy metals by newer, therapeutically useful chelating agents. Toxicology. 1995;97(1-3):23-38. 8. Aposhian HV, Bruce DC, Alter W, Dart RC, Hurlbut KM, Aposhian MM. Urinary mercury after administration of 2,3-dimercaptopropane-1-sulfonic acid: correlation with dental amalgam score. FASEB J. 1992;6(7):2472-6. 9. Aaseth J, Skaug MA, Cao Y, Andersen O. Chelation in metal intoxication-Principles and paradigms. J Trace Elem Med Biol. 2014; 10. Cao Y, Skaug MA, Andersen O, Aaseth J. Chelation therapy in intoxications with mercury, lead and copper. J Trace Elem Med Biol. 2014; 11. Nielsen JB, Andersen O. Effect of four thiol-containing chelators on disposition of orally administered mercuric chloride. Hum Exp Toxicol. 1991; 10: 423-430. 12. Planas-bohne F. The effect of 2,3-dimercaptorpropane-1-sulfonate and dimercaptosuccinic acid on the distribution and excretion of mercuric chloride in rats. Toxicology. 1981;19(3):275-8. 13. Clarkson TW, Magos L, Cox C, et al. Tests of efficacy of antidotes for removal of methylmercury in human poisoning during the Iraq outbreak. J Pharmacol Exp Ther. 1981;218(1):74-83. 14. Ruha AM. Recommendations for provoked challenge urine testing. J Med Toxicol. 2013;9(4):318-25. 15. Bates N. Metallic and inorganic mercury poisoning. Emerg Nurse. 2003;11(1):25-31. 16. Guha mazumder DN, De BK, Santra A, et al. Randomized placebo-controlled trial of 2,3-dimercapto-1-propanesulfonate (DMPS) in therapy of chronic arsenicosis due to drinking arsenic-contaminated water. J Toxicol Clin Toxicol. 2001;39(7):665-74. 17. Muran PJ. Mercury elimination with oral DMPS, DMSA, vitamin C, and glutathione: an observational clinical review. Altern Ther Health Med. 2006;12(3):70-5. 18. .Rooney JP. The role of thiols, dithiols, nutritional factors and interacting ligands in the toxicology of mercury. Toxicology. 2007;234(3):145-56.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Toxicology Blog
AuthorEM Rotators on Toxicology Selected by Feedspot as one of the Top 20 Toxicology Blogs on the web
Archives
March 2018
Categories
All
Disclaimer: All images included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
