|
I wanted to clarify that the previous critical care billing card posted is a reference as a reminder that you *may* have performed critical care. It is not an absolute "if A then B." As per usual, your documentation must support that you spent 31 minutes or greater solely dedicated to the care of the patient and that they had a critical organ or life threat. In reference to the previously posted critical care card, our coding support team has identified a few items that alone would not be sufficient to claim critical care:
They have provided us with MedData's "Critical Care Descriptors: Description that highly suggest critical care" PDF that I have attached. Please reference this PDF as well. REMEMBER: THESE ARE ONLY REMINDERS THAT ARE HIGHLY SUGGESTIVE THAT YOU PERFORMED CRITICAL CARE. YOUR DOCUMENTATION MUST ALSO REFLECT THAT YOU SPENT A DEDICATED >31 MINUTES SOLEY ON THE PATIENT'S CARE.
0 Comments
As previously covered, critical care billing is often overlooked in documentation, even when it performed. Many don't know the breadth of diagnoses and interventions that can justify this billing. The below card lists diagnoses, interventions and medications that justify the documentation and billing of critical care.  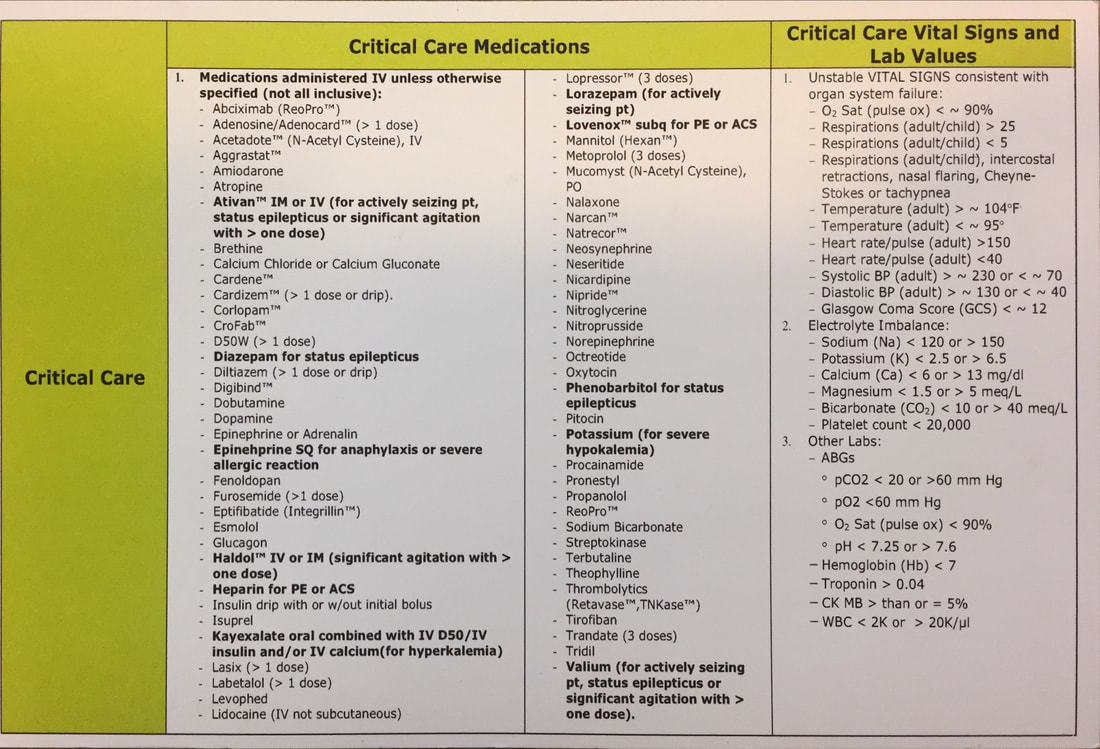 Gentle reminder!
"Negative" or "No Significant Past Medical History" are not acceptable phrases for Medicare billing for Past Medical History/Surgical History/Family Hisotry/Social History. BAD: Negative BAD: No Significant Past Medical History BAD: Denies BAD: Not Significant BAD: Reviewed in Chart GOOD: Denies Past Medical History GOOD: No Past Medical History GOOD: See HPI / See Problem List ** (caveat: you must reference PMHx in the history, avoid the word significant) Specific TIME is an important component of critical care billing. BAD: 30-74 minutes of critical care performed GOOD: In excess of 30 minutes of critical care performed GOOD: x Minutes of critical care performed GOOD: In excess of 74 minutes of critical care performed Don't Forget: to add "excluding teaching time or time performing procedures" That's a wrap folks. We are doing better but I have seen SEVERAL slip ups on the past medical history issue. Like it or not ICD-10 was introduced by CMS last year. Medicare has given a 1 year "grace" period to be more compliant with ICD-10 appropriate diagnoses. This grace period ends October 1, 2016.
We have been reminded to be "as specific as possible" when selecting our diagnoses. If the documentation supports a specific ICD-10 code, that diagnosis should be chosen. Sometimes, the unspecified code is all we may be able to diagnose. That is acceptable if our documentation supports that there is not enough clinical information to support a specific code. EXAMPLES BAD: Laceration GOOD: Facial Laceration BAD: Abdominal pain GOOD: Acute right lower quadrant pain BAD: Chest Pain GOOD: Acute chest pain BETTER: Chest wall pain THIS IS NOT LIMITED TO CHS. This is mandated by Centers for Medicare and Medicaid Services (CMS) One of our jobs with documenting is to help the coders bill our services to the appropriate level of service we provide. As tempting as it is to be frustrated by this, more often than not, charts and reimbursement are being under-coded. YOU can help by being thoughtful with the diagnoses you select. My legal risk tolerance is to leave diagnoses unspecified if the exact cause is unknown. I frequently use "Chest Pain" as a diagnosis. I commonly document "that the exact etiology of the patient's [chest pain] is unclear." I will almost always add this statement to my undifferentiated patients of high risk. I expect that this post will generate a good discussion on charting tips for our large subset of patients with unclear diagnoses. I'm looking forward to hearing what other folks will document to help our coders be compliant with ICD-10. It's been several months since the last post. I hope you haven't forgotten the pearls I've previously posted. This is a good time to review my previous posts for a quick refresher. Now is a great time to talk about critical care billing. There has been a substantial change in what our coders will allow to be documented. SUMMARY OF DOCUMENTING PEARLS
3 ELEMENTS OF CRITICAL CARE
KEY DOCUMENTATION REQUIREMENTS
MEDICARE REQUIREMENTS FOR TEACHING ATTESTATIONS
Finally, I've included the following table outlining RVU compensation as a reminder of why documenting is so important. Critical care billing increased RVU generation by approximately 25% over a Level 5 chart. 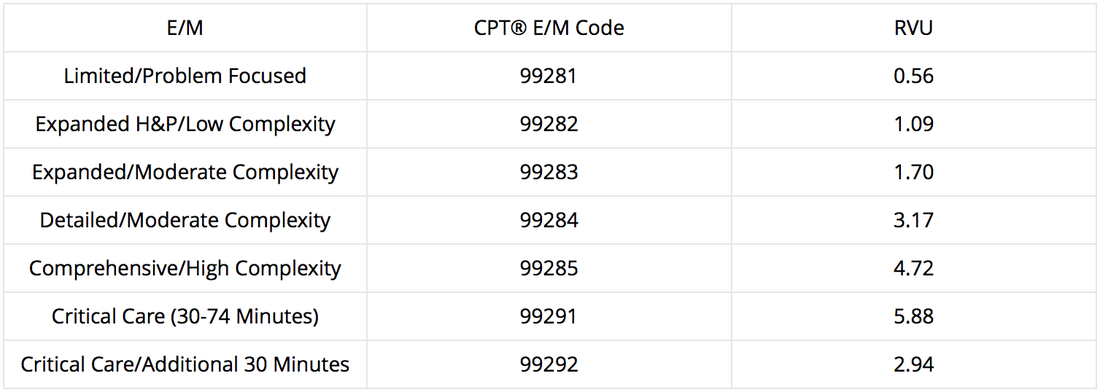 A few questions were raised after the last post, I've included this for everyone's benefit.
Q: What do you suggest for Family History when the Family History is unrelated to the patient's problem? A: Medicare likes the PMFSH (Past Medical/Family/Social History) section to be as specific as possible. So, statements like "No Significant Family History" are not adequate. Strictly from a billing standpoint, documenting unrelated family history counts. A medico-legally sound approach to family history is to document pertinent negatives. For example, for headache patients documenting "No family history of aneurysm" is not only billable, but medico-legally sound. Another example would be for chest pain patients. Documenting " No family history of early CAD, MI, TAD" is billable and is an excellent way to document your risk stratification analysis. Q: What about documenting under PMFSH - "Please refer to HPI." Is this ok? A: Technically it is adequate IF you actually include PMFSH in the HPI. I have seen "Please refer to HPI" used but no mention of a patient's past medical or social history is actually included in the HPI. That DOES NOT COUNT. Remember: you want to make the job as easy as possible for the billers to not inappropriately down code your chart. My personal preference is to not use "Please refer to HPI" and document in the designated sections to assist with billing. It's still ok to include past medical history in the HPI, however. Q: I'm confused, I thought you said "Negative" was allowed! A: Nope! You are mistaken. "Negative" "Non-Contributory" "No Significant PMHx" "None" "Denies" "Reviewed in chart" are not adequate phrases. It's an easy fix: make a macro that says "No Past Medical History" Coming up: Top 5 documenting foils! Another word on Past Medical & Surgical History, Family History, Social History:
One of the most likely places to get down coded is in this section of your chart. I've outlined the numbers before, but overlooking this portion of the chart is EASY to do. Over the past 2 months, I've seen this section be improperly documented on almost every single shift by all level EM residents.
Acceptable phrases include "Denies Past Medical History" & "No Past Medical History" High Acuity Caveat will allow you to use the phrase "Unknown" however your chart has to clearly describe why High Acuity Caveat applies and why you were unable to obtain these historical elements. REMEMBER: Coders can only bill for services that are provided AND documented. Welcome Interns!
You are no longer medical students. Congratulations!! That being said, your chart actually matters (from a billing perspective). This is a great time to start habits to chart effectively/efficiently. Basic Documenting Concepts CPT CODE There are 5 levels of ER chart coding based on your documentation; these are called CPT codes. Level 1 being the most basic, Level 5 being the most complex. (Billing follows closely, 1 pays the least, 5 pays the most). RVU - "Relative Value Unit" Your reimbursement is based on the number RVU's you generate. You generate RVU's by your ER documentation, performing and documenting procedures, and performing and documenting critical care. Each CPT code correlates with a fixed amount of RVU's. Level 1 chart = 0.59 RVU Level 2 chart = 1.16 RVU Level 3 chart = 1.75 RVU Level 4 chart = 3.33 RVU Level 5 chart = 4.93 RVU Critical Care 1st hour = 6.33 RVU Critical Care each additional 30 minutes = 3.16 RVU Missing key documenting elements can easily drop a chart from a Level 5 to a Level 3. As you can see, this is over 3 RVUs! Components of the Document History - There are 4 subcomponents:
Exam
MDM (medical decision making)
Putting it all together (CPT LEVEL CODING) LEVELS:
COMMON PITFALLS
This is a brief introduction into mastering charting. Your charts should be a thoughtful representation of the work you performed. Be mindful when using Dragon Dictation that you've included the elements needed to support the work that you are already doing. Stay tuned for more tips (and feel free to review my previous blog posts)! 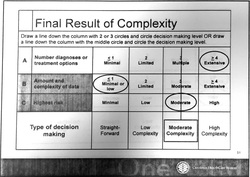 What is MDM from a billing perspective? Documentation is VERY important. Coders are looking for specific things. I'll provide a quick summary read on for more specifics. Summary Tips: 1. Avoid statements like "We'll go ahead and order..." INSTEAD document labs/xrays/ct findings 2. Document interventions - IV Fluids, and IV or PO medications given, and prescribed medications at discharge. 3. Document review of past medical records and document at least 1 pertinent finding. 4. Document consults with physicians and context of conversations. From a legal standpoint, I personally believe you should ALWAYS do this as well as the time of conversation. 5. Document personal review of images (click box EP interpretation) 6. Document timed re-evaluations. 7. Do not include definition of criteria (NEXUS, Canadian C-spine, PERC, etc..). This is NOT MDM and makes the chart difficult to dissect for pertinent information. Don't get macro happy. 8. Avoid lengthy paragraphs that buries billable information. Make it easy for the coders to see. Want more? Coders calculate MDM complexity via a point system. The MDM formula is a summation of: A: Number of diagnoses or treatment options B: Amount and/or complexity of data C: Risk associated with patient's condition A: Number of diagnoses or treatment options: In the ER, it is assumed that the problem is new to the examiner. We get 3 points for no additional workup and 4 points for additional workup B: Amount and/or Complexity of Data to be reviewed: *** The coders have been clear that discussing the tests that you are going to order does not factor into medical decision making points. Specifically, MDM including phrases "we're going to order XXX" are not factored in MDM points. *** They consider the data reviewed, discussions held about the patient, and test ordered during the encounter. The more data addressed during the encounter, the more complex the decision-making. Factors that do get "MDM points" 1.(1pt) Review of clinical lab tests 2.(1pt) Review of radiology tests 3.(1pt) Review of EKG Refer to EKG blog post for billing tips 4.(1pt) Discussion of test results with consulting physicians Discussion of case with another provider must document what was discussed briefly (i.e. will admit, agree with antibiotics, will see in follow up, etc...) 5. (1pt) Decision to obtain old records/obtain supplementary history (from someone other than patient) 6. (2pts) Review and summarization of old records and/or history AND/OR discussion of case with another healthcare provider Include a brief summary of relevant information. This can be as simple as baseline creatinine, previous EF, results of recent stress test, etc... 7. (2pts) Independent visualization of image or tracing. "Personal review of image shows...." C: Risk associated with patient's condition: It is not obvious to coders what interventions have been performed. The coders do not have access to the MAR to see what medications have been given. Specifically, IV fluids, IV/PO narcotics, pressors, IV cardiac meds, and prescribed medications increase complexity. If evaluating and treating an ongoing problem, clearly document the severity of the problem during that encounter. See insert below. CALCULATE THE MDM: See the graphic to the right.. Complexity gets determined by the 2 of 3 rule. Line is drawn and complexity of MDM is determined by the level which captures at least 2 of 3 factors. Reference: Faculty Reimbursement Coders Education: E/M Coding, Corporate Compliance March 14,2014 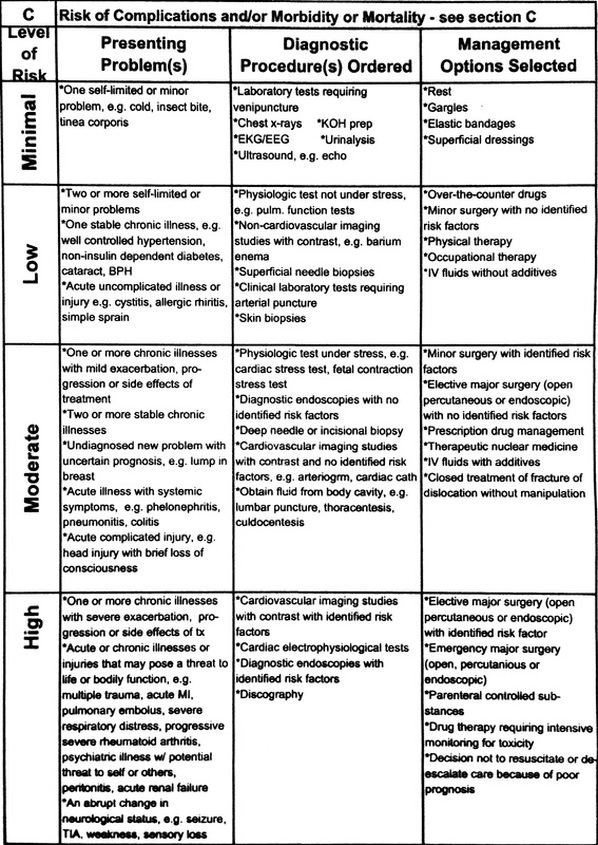 Procedural Sedation Documentation Pearls
Our ER notes need to clearly document the sedation time. Referring to RN notes is not adequete as it is difficult for coders to follow the flow sheet accurately. For a Procedural Sedation to be billable, "intraservice" sedation time documented needs to be at least 16 minutes. "Moderate sedation is a time based code. Because the Moderate Sedation codes indicate a unit of time of 30 minutes, the ED chart must indicate 16 minutes or more of intraservice time to report Moderate Sedation. If the time threshold has not been met, then the code is not reportable." - Oct 2011 CPT Assistant Units of time billable for procedural sedation are: Per CPT, a unit of time is attained when the midpoint has been passed. Initial 30 minutes (must document at least 16 minutes to get reimbursed) Each addition 15 minutes can be billed. Must document at least 37.5 minutes for up to 45 minutes [30 min unit + one 15 min unit]; Must document at least 52.5 minutes for up to 60 minutes [30 min unit + two 15 min units], etc... Intraservice time is defined as: Starts with the administration of the sedation agent(s) Requires continuous face-to-face attendance Ends at the conclusion of personal contact by the physician providing the sedation. Other Pearls: Documentation should include the name of the procedure, medication names, dosages and routes of administration, who administered the medication(s) (physician or observer), notations of ongoing assessments and vital signs monitoring during moderate sedation. Using the Procedural Sedation sentence in PowerNote includes all of these elements. Nilesh |
Coding blog
Archives
August 2017
Categories
All
Disclaimer: Information contained in this blog is the opinion of the author and does not necessarily reflect the official opinion of Carolinas HealthCare System. Application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
