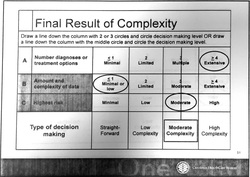
 What is MDM from a billing perspective? Documentation is VERY important. Coders are looking for specific things. I'll provide a quick summary read on for more specifics. Summary Tips: 1. Avoid statements like "We'll go ahead and order..." INSTEAD document labs/xrays/ct findings 2. Document interventions - IV Fluids, and IV or PO medications given, and prescribed medications at discharge. 3. Document review of past medical records and document at least 1 pertinent finding. 4. Document consults with physicians and context of conversations. From a legal standpoint, I personally believe you should ALWAYS do this as well as the time of conversation. 5. Document personal review of images (click box EP interpretation) 6. Document timed re-evaluations. 7. Do not include definition of criteria (NEXUS, Canadian C-spine, PERC, etc..). This is NOT MDM and makes the chart difficult to dissect for pertinent information. Don't get macro happy. 8. Avoid lengthy paragraphs that buries billable information. Make it easy for the coders to see. Want more? Coders calculate MDM complexity via a point system. The MDM formula is a summation of: A: Number of diagnoses or treatment options B: Amount and/or complexity of data C: Risk associated with patient's condition A: Number of diagnoses or treatment options: In the ER, it is assumed that the problem is new to the examiner. We get 3 points for no additional workup and 4 points for additional workup B: Amount and/or Complexity of Data to be reviewed: *** The coders have been clear that discussing the tests that you are going to order does not factor into medical decision making points. Specifically, MDM including phrases "we're going to order XXX" are not factored in MDM points. *** They consider the data reviewed, discussions held about the patient, and test ordered during the encounter. The more data addressed during the encounter, the more complex the decision-making. Factors that do get "MDM points" 1.(1pt) Review of clinical lab tests 2.(1pt) Review of radiology tests 3.(1pt) Review of EKG Refer to EKG blog post for billing tips 4.(1pt) Discussion of test results with consulting physicians Discussion of case with another provider must document what was discussed briefly (i.e. will admit, agree with antibiotics, will see in follow up, etc...) 5. (1pt) Decision to obtain old records/obtain supplementary history (from someone other than patient) 6. (2pts) Review and summarization of old records and/or history AND/OR discussion of case with another healthcare provider Include a brief summary of relevant information. This can be as simple as baseline creatinine, previous EF, results of recent stress test, etc... 7. (2pts) Independent visualization of image or tracing. "Personal review of image shows...." C: Risk associated with patient's condition: It is not obvious to coders what interventions have been performed. The coders do not have access to the MAR to see what medications have been given. Specifically, IV fluids, IV/PO narcotics, pressors, IV cardiac meds, and prescribed medications increase complexity. If evaluating and treating an ongoing problem, clearly document the severity of the problem during that encounter. See insert below. CALCULATE THE MDM: See the graphic to the right.. Complexity gets determined by the 2 of 3 rule. Line is drawn and complexity of MDM is determined by the level which captures at least 2 of 3 factors. Reference: Faculty Reimbursement Coders Education: E/M Coding, Corporate Compliance March 14,2014 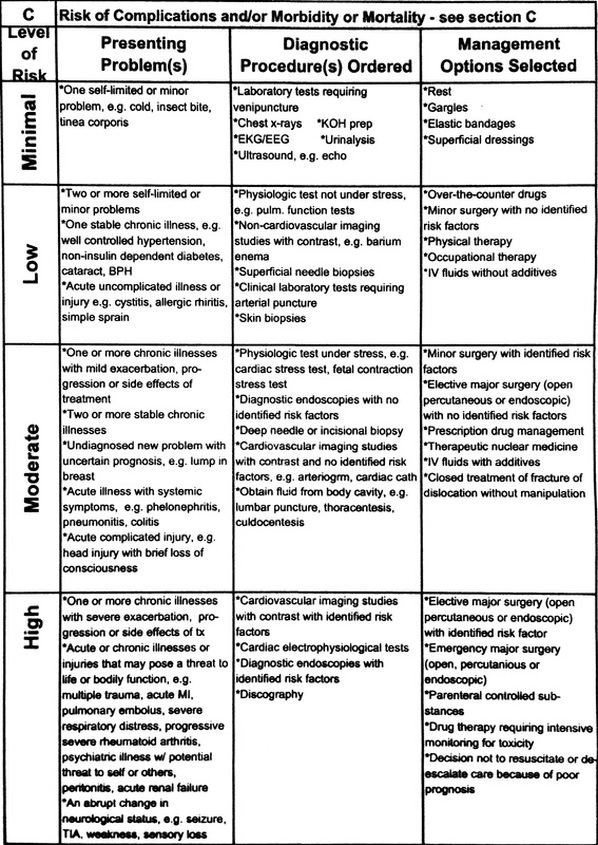
0 Comments
|
Coding blog
Archives
August 2017
Categories
All
Disclaimer: Information contained in this blog is the opinion of the author and does not necessarily reflect the official opinion of Carolinas HealthCare System. Application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
