|
It's been several months since the last post. I hope you haven't forgotten the pearls I've previously posted. This is a good time to review my previous posts for a quick refresher. Now is a great time to talk about critical care billing. There has been a substantial change in what our coders will allow to be documented. SUMMARY OF DOCUMENTING PEARLS
3 ELEMENTS OF CRITICAL CARE
KEY DOCUMENTATION REQUIREMENTS
MEDICARE REQUIREMENTS FOR TEACHING ATTESTATIONS
Finally, I've included the following table outlining RVU compensation as a reminder of why documenting is so important. Critical care billing increased RVU generation by approximately 25% over a Level 5 chart. 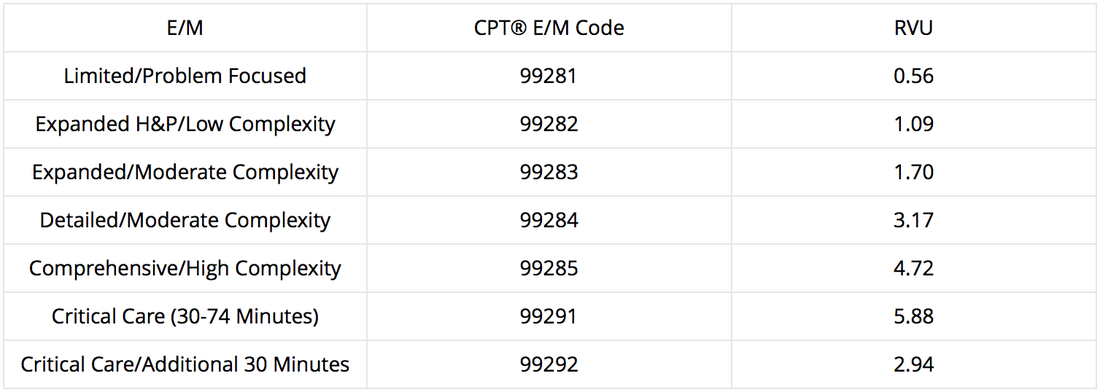
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Coding blog
Archives
August 2017
Categories
All
Disclaimer: Information contained in this blog is the opinion of the author and does not necessarily reflect the official opinion of Carolinas HealthCare System. Application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
