|
HPI: This is a full-term 2 week female infant here with 4 episodes of bright red blood mixed with her stool over 24 hours. Last episode occurred in the examination room. She has continued to breast feed well with no fevers, vomiting, weight loss, abdominal pair, or irritability. Birth History: Mom was 26yrs, G1P1. Birth weight 3.1 kg. SVD and GBS negative. Received vitamin K at birth. Born in hospital and had pre-natal care. All serologies negative. Physical Exam: Afebrile and all vital signs are within normal limits. Wt 3.2kg. Well appearing. Abdomen is soft, non-distended, non-tender with normal bowel sounds. No hepatosplenomegaly. Normal external female genitalia. No anal fissures/tears/skin tags visualized. Normal rectal tone. Stool in diaper is yellow and seedy with blood mixed throughout (guaiac positive). Mom has a normal breast exam without signs of fissures or active bleeding. 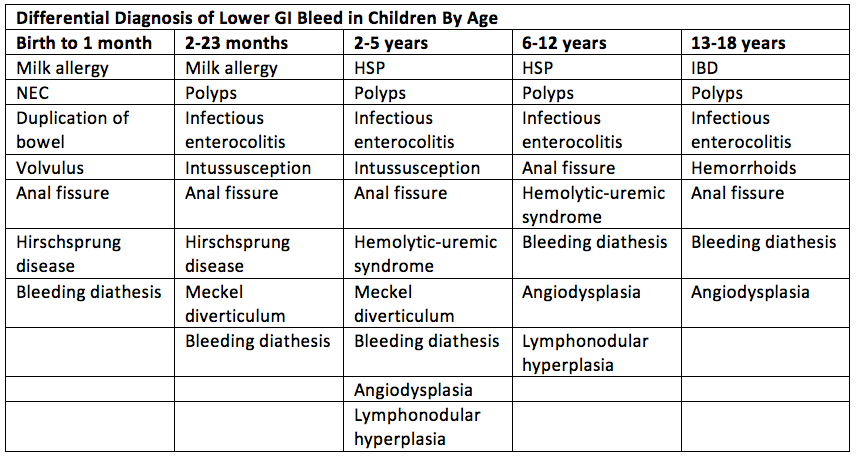 Work-up:
- Thorough history and physical exam o Age of patient o Diet o NSAID use o Color of blood (Bright red blood, maroon stools, dark tarry stools, etc) – i.e. is it upper GI or lower GI o Volume of blood and how often it occurs o Associated symptoms o Palpation of a polyp on rectal exam, anal fissures, anal tears? - Hemoccult (false-negative and false-positives are possible) – i.e. is it blood? - Apt-Downey test may help distinguish between fetal and maternal blood (swallowed blood during delivery or fissured maternal breast with feeding) - CBC with diff (and serial hemoglobin levels with admission) level - Consider coagulation studies, liver function tests, and stool evaluation (C. diff) - Cross and match if profuse bleeding - Consider supine, upright, and lateral decubitus abdominal radiographs to evaluate for air-fluid levels, dilated loops of bowel, pneumoperitoneum, or pneumatosis - Additionally radiographic imaging should be directed by your history and physical – i.e. an upper GI with small bowel follow-through if concerned about malrotation, ultrasound for possible intussusception, etc. Management: - Cardiopulmonary and fluid resuscitation as needed (with crystalloid or colloid as needed) - Consider a surgery consult if concern for surgical entity such as NEC - Consider broad-spectrum antibiotics if concern for an acute abdomen or sepsis - Consider NG tube placement for gastric decompression - Admission unless clear benign source and they have good follow-up - May require GI consult or hematology consult on admission as indicated Discussion: - Lower GI bleeds account for 30% of cases of GI bleeding presenting to the ED - Hematochezia is usually a manifestation of bleeding from the distal small bowel or proximal colon but can represent severe upper GI bleed - Often benign and self-limited but can represent serious illness and is very anxiety provoking in parents/physicians - Red Kool-Aid, red gelatin, fruit punch, tomato/cranberry juice, beets, peach skin, rifampin, medications with red syrup may lead to red appearing stool - Eosinophilia may indicate milk protein allergy - 10% of cases of necrotizing enterocolitis present in full-term infants and may present with non-specific symptoms and blood in the stool - Melena may occur with malrotation and volvulus when vascular compromise occurs – 10-20% of the time - 25% of patients with Hirschsprung related enterocolitis will present with blood in the stool - Changing to an elemental formula like alimentum or nutramigen if concerned about milk-protein allergy Patient Course This 2 week old was noted to have mild abdominal distention on re-examination and had an additional 3 episodes of hematochezia in the ED. A KUB with lateral decubitus view was ordered and radiology reported questionable signs of pneumatosis. Surgery was consulted who felt she was fussy and requested an abdominal ultrasound which was negative for intussusception. At that time, the patient was hospitalized with CHIPS and a surgical consult. Coagulation studies were obtained and she was found to have a greatly prolonged PT and aPTT. Hematology was consulted who recommended a coagulation work-up in addition to repeating the PT and aPTT. These were normal and it was felt the initial laboratory values were in error. GI was consulted as well and patient was ultimately discharged home with a diagnosis of milk-protein allergy and is doing well on an elemental formula. By Jeremiah Smith, MD References
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Pediatric EM Blog
AuthorPediatric EM Fellows at CMC/Levine Children's Hospital. Archives
November 2016
Categories
All
Disclaimer: All images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
