|
By Christyn Magill MD CC: infant vomiting HPI: 2mo term female, born at 38 weeks gestation, SVD, no complications, normal prenatal labs. Presents with 3 days of projectile vomiting about 10-15 minutes after feeds. Initially vomitus appeared to be regurgitated food. Now, vomitus is darker in color, but no bright red blood, non bilious. Decreased UOP. Normal bowel movements per parents. Normal energy. Acting hungry. Parents deny fevers, sick contacts, rashes, diarrhea. Vomiting seems to bother child and gets fussy, but acts normally in between feeds. This is a first child for the family. Physical Exam: VS: T 98.6F rectal, HR 135, BP 114/74, RR 44, O2 98% on RA GENERAL: Laughs and smiles, very active in the ED, not clinically dehydrated HEENT: PERRL, EOMI, moist mucous membranes, no icterus, TM's NL, Oral-pharynx NL, nares NL CHEST: Normal S1 and S2, no murmurs, lungs clear to auscultation ABD: Tenderness-none, no HSM, bowel sounds NL Rectal: normal tone, small amt stool in vault, Hemoccult-positive stool BACK: Non tender, no costovertebral angle tenderness EXTREMITY: Normal active full ROM throughout all extremities, no tenderness, appearance normal GU: Normal external female genitalia SKIN: No pallor/rashes, warm & moist, brisk cap refill NEURO: Good suck, grasp, makes eye contact, social smile, +Moro reflex, Gross motor normal, gross sensation intact LYMPH: No lymphadenopathy What is on your differential diagnosis? What is your highest suspicion? What studies would you do on this patient in the ED? The following studies were done: VBG: pH 7.418, PCO2 28.8, PO2 49, Lactate 2.87, HCO3 18.6, Base deficit 5 Urine dip: glu-neg, bili-neg, ketones-large (80), SG-1.030, pH 6.0, prot-1+, urobil-normal, nitrate- neg, leuk-neg CBC: WBC 13.4K, Hb 10.9, Hct 32%, Plt 430 Chem8: Na 137, K 4.8, Cl 103, CO2 18, BUN 10, Cr <0.2, Glu 90 Hepatic: TProtein 5.4, Albumin 4.0, TBili 1.2, Dbili 0.2, Alk Phos 344, ALT 24, AST 34 CRP <0.5 Imaging: 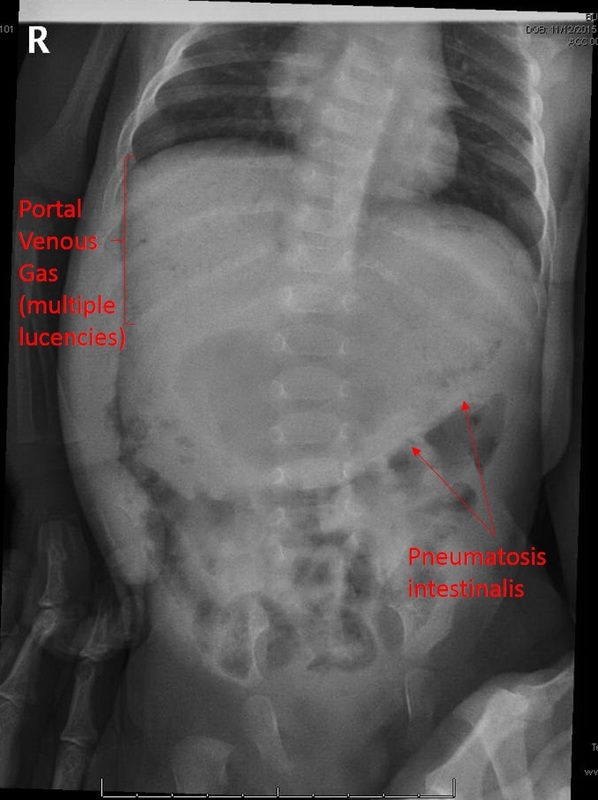 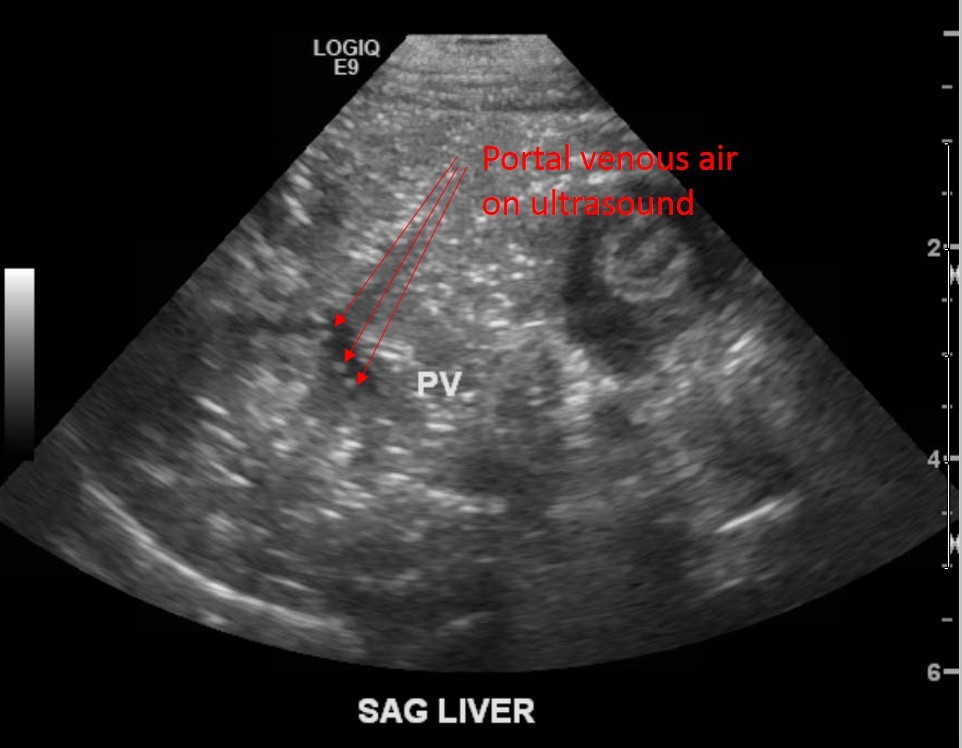 What is your diagnosis based on these studies? What is your management? Diagnosis: Necrotizing Enterocolitis Clinical Question: How do I recognize this in the emergency department, and what do I do about it? Helpful hint: http://pedemmorsels.com/necrotizing-enterocolitis/ Discussion:[1, 2]
Pathology
Epidemiology- Often, but not always, the term babies who develop NEC have some sort of underlying abnormality.[4-6]
Usually presents earlier in term babies- In one retrospective study done by Sharma et al, the extremely premature infants presented with symptoms of NEC an average of 22 days of life, whereas the term babies had symptoms an average of 3 DOL. But this is not always true, as was the case with our baby above. Symptoms/Stages Modified Bell’s Criteria From Up To Date: 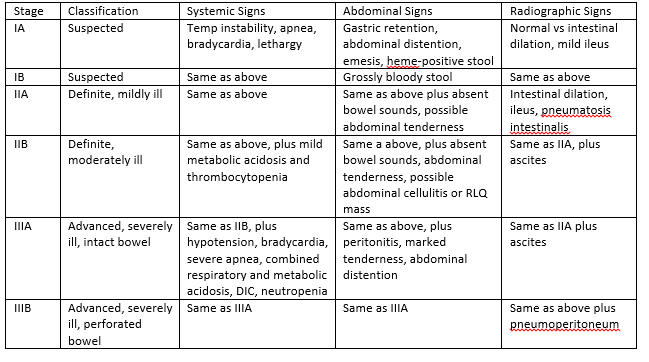 Workup[2]
CBC plus diff, BMP, LFTs (if more advanced stages), VBG Thrombocytopenia, metabolic acidosis, hyperglycemia are trended for worsening disease. Plain films- upright and lateral decubitus to eval for free air, pneumatosis intestinalis, portal venous gas. RUQ Ultrasound to show portal venous gas. [7] Treatment[8] Medical- Antibiotics, bowel rest, supportive care, lab and radiologic monitoring. Antibiotic possible regimens (from UTD): ●Ampicillin, gentamicin (or amikacin), and metronidazole ●Ampicillin, gentamicin (or amikacin), and clindamycin ●Ampicillin, cefotaxime, and metronidazole ●Piperacillin-tazobactam and gentamicin (or amikacin) ●Vancomycin, piperacillin-tazobactam, and gentamicin ●Meropenem *Vancomycin instead of Ampicillin if in high MRSA area *Add Fluconazole if worried about fungal infection Surgical[9, 10]
Complications[6, 11] Acute- sepsis, meningitis, peritonitis, abscess formation, DIC, hypotension, shock, respiratory failure, hypoglycemia, metabolic acidosis Late- intestinal stricture, short gut syndrome *intestinal strictures in 9-36%, not significantly related to medical vs surgical treatment, drain vs laparotomy, gestational age, pneumatosis intestinalis. Term infants- 3% risk of NEC, 16% mortality. Updates Probiotics are now being studied for protective potential. [5] Back to our patient:
Clinical Pearls for ED:
References: 1. Sakellaris, G., et al., Gastrointestinal perforations in neonatal period: experience over 10 years. Pediatr Emerg Care, 2012. 28(9): p. 886-8. 2. Solomkin, J.S., et al., Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis, 2010. 50(2): p. 133-64. 3. Sharma, R., et al., Impact of gestational age on the clinical presentation and surgical outcome of necrotizing enterocolitis. J Perinatol, 2006. 26(6): p. 342-7. 4. Short, S.S., et al., Late onset of necrotizing enterocolitis in the full-term infant is associated with increased mortality: results from a two-center analysis. J Pediatr Surg, 2014. 49(6): p. 950-3. 5. Terrin, G., A. Scipione, and M. De Curtis, Update in pathogenesis and prospective in treatment of necrotizing enterocolitis. Biomed Res Int, 2014. 2014: p. 543765. 6. Lambert, D.K., et al., Necrotizing enterocolitis in term neonates: data from a multihospital health-care system. J Perinatol, 2007. 27(7): p. 437-43. 7. Buonomo, C., The radiology of necrotizing enterocolitis. Radiol Clin North Am, 1999. 37(6): p. 1187-98, vii. 8. Barie, P.S., et al., A randomized, double-blind clinical trial comparing cefepime plus metronidazole with imipenem-cilastatin in the treatment of complicated intra-abdominal infections. Cefepime Intra-abdominal Infection Study Group. Arch Surg, 1997. 132(12): p. 1294-302. 9. Flake, A.W., Necrotizing enterocolitis in preterm infants--is laparotomy necessary? N Engl J Med, 2006. 354(21): p. 2275-6. 10. Moore, T.C., Successful use of the "patch, drain, and wait" laparotomy approach to perforated necrotizing enterocolitis: is hypoxia-triggered "good angiogenesis" involved? Pediatr Surg Int, 2000. 16(5-6): p. 356-63. 11. Schwartz, M.Z., et al., Intestinal stenosis following successful medical management of necrotizing enterocolitis. J Pediatr Surg, 1980. 15(6): p. 890-9.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Pediatric EM Blog
AuthorPediatric EM Fellows at CMC/Levine Children's Hospital. Archives
November 2016
Categories
All
Disclaimer: All images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
