|
HPI: young male s/p ATV accident Exam: Inspection: edema and deformity. No open wounds. Palpation: TTP, palpable deformity. 2+ DP/PT pulses. SILT lower extremity. ROM: unable to perform straight leg raise. limited ROM secondary to pain. Limited assessment of anterior/posterior drawer, varus/valgus testing Imaging: # Best seen on lateral xray. #In pediatric patients, MRI if xrays do not show fracture and child unable to perform straight leg raise   orthobullets.com orthobullets.com Bipartate patella: #often mistaken for fracture-use history and clinical exam #8-10 % of population, 50 % bilateral, usually superolateral Fracture Patterns:
Management: # Nonoperative: -Extensor mechanism intact (straight leg test) -nondisplaced/minimally displaced -vertical fractures -Knee immobilized in extension (cylinder cast/brace) #Operative -extensor mechanism failure -open fractures -articular displacement > 2 mm -displacement > 3 mm -patella sleeve fractures in children (fracture between cartilage sleeve and patella) -severely communited fractures Discussion: -Patella fractures 1 % of skeletal injuries -Mechanism: direct impact of indirect eccentric contraction -Complications: weakness and anterior knee pain, loss of reduction, nonunion, osteonecrosis, infection, stiffness Key Points: #History of mechanism and exam is important-especially palpation, straight leg testing #Best seen on lateral xray, consider MRI in pediatric patients given history and exam findings #Bipartate patella-seen in 8-10 % of population, usually superolateral #Orthopedic consultation-open vs closed, fracture pattern, straight leg testing, displacement #Consider patella sleeve fractures in pediatric patients #Management-minimally displaced, vertical, closed, extensor mechanism intact-immobilize in brace or cast and follow up as outpatient; Open, extensor mechanism not intact, communited, displaced-surgical
0 Comments
HPI: Toddler with history of osteogenesis imperfecta type 1 presented after a fall resulting in bruising to right lower extremity, fussiness. Exam: vs normal 5 cm bruise to mid right shin, 2+ DP/PT pulses, cap refill < 2 sec. Full range of motion at hip, knee and ankle joint. Intact plantar, dorsiflexion, leg extension. NO laxity or pain with valgus or varus stress testing. Imaging: -Require AP and lateral views of tibia and fibula, ipsilateral knee and ankle -Imaging below shows a non-displaced spiral tibial shaft fracture  Management:
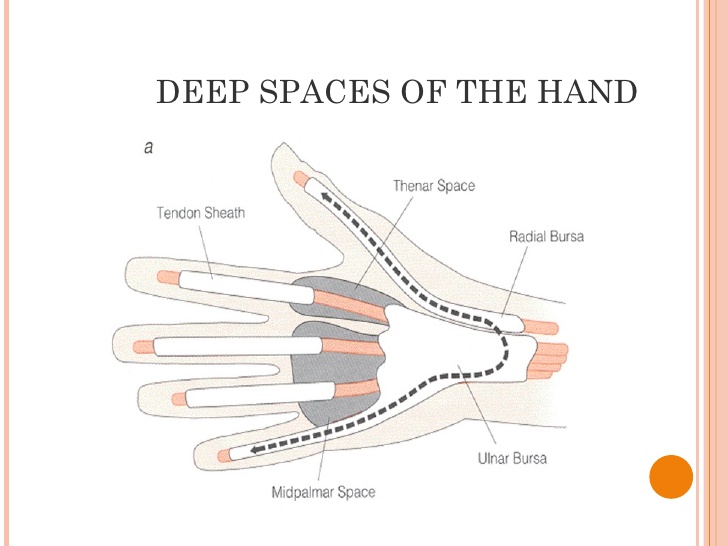
-Closed reduction with long leg cast -Follow up with orthopedics in 2 weeks Anatomy: -Distal half of tibia, fibula usually remains intact Discussion: -15 % of all pediatric fractures -If not walking yet, consider NAT -May present with bruising, limping, refusal to bear weight -Mechanism usually low energy with rotation Key Points: -Toddler fractures common (15 %) -Consider NAT if not walking yet -AKA childhood accidental spiral tibia (CAST) fractures -MOI: low energy, rotation -History: pain, limp, not bearing weight -Exam: warmth, pain, bruising, pain with ankle dorsiflexion -Obtain: xrays AP/lateral tibia/fibula, ipsilateral knee and ankle -Manage with closed reduction and long leg cast with orthopedic follow up in 2 weeks -Prognosis: good, usually heal in 3-4 weeks -Complications: compartment syndrome, leg-length discrepancy, angular deformity HPI: Teenage RHD healthy male presented initially to PCP with blister to left hand from playing baseball. Small blister incised and culture sent which eventually grew out MRSA and he was started on bactrim. On follow up 4 days later swelling worsened with worsening surrounding erythema. Denied fevers ,chills or other symptoms. Denied insect, spider or other exposures. Admitted for IV antibiotics and ortho hand consultation. Exam: afebrile, vitals normal 2+ radial pulse, cap refill < 2 sec SILT throughout hand and digits Flexion/Extension/adduction/abduction intact and notable only for mild pain with flexion of thumb, area of fluctuance to radial aspect of palm extending from mid palm around to dosal aspect of 1st and 2nd digits; see picture
Imaging:
Management: Orthopedic hand consultation Admission for IV antibiotics
Anatomy: 3 main deep spaces: potential spaces separated by fascial septum
Key Points:
By: Dr Bryon Callahan
HPI: Right hand dominant middle aged female with history of HTN presents to the ED after accidentally hitting her left index finger with a hammer while working on a home improvement project. Finger is painful and swollen but she has no other injuries and reports she is otherwise feeling well. Physical Examination: Erythematous, swollen, and tender left 2nd distal phalanx. There is a subungual hematoma present over approx. 75% of the nail but the nail is intact. Motor and sensation intact, full ROM of PIP and DIP, 2+ radial pulse, no other injuries identified. Radiology: AP, lateral and oblique views of left 2nd phalanx – no fracture or dislocation identified Management: Nail removal and bedside repair of nail bed laceration, tetanus updated, discharged home with 48 hour follow up for reevaluation Discussion: Fingertip injuries = most common hand injuries seen in the ED Most common mechanisms:
Evaluate for:
Complications of injury:
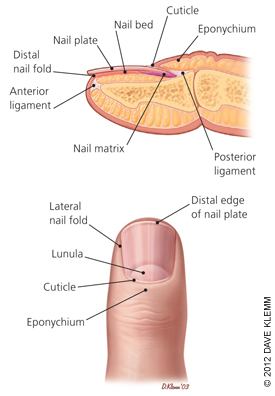 Image obtained from Am Fam Physician. 2012 Apr 15;85(8):779-787. Fingertip Anatomy:
Blood Supply and Innervation:
Nail Growth:
Treatment: Obtain radiographs to rule out distal phalanx fracture Evaluate for subunginal hematoma and nail bed lacerations Drain hematoma if <50% nail involved
Nail removal, I&D, repair of nail bed if >50% of nail involved
HPI: 20ish year old and otherwise healthy male presents as the restrained driver in head-on MVC at low speed just prior to arrival. He has a large linear laceration to anterior aspect of R knee and is unable to fully extend the knee. Wound is hemostatic. No other injuries or complaints. Physical Examination: 10cm linear, horizontal laceration to the anterior aspect of the patient’s R knee. Knee is held in slightly flexed positioning. Decreased ROM of the knee secondary to pain and injury, patient unable to actively extend extremity in straight leg raise. FROM of ankle. 2+ DP and PT pulses present. Sensation intact to light touch throughout. No erythema, swelling or significant tenderness present over RLE. Radiology: AP/Lateral/Sunrise/Oblique views of R knee: Transverse fracture of the patella with 3mm of displacement present and surrounding soft tissue edema Management:
Discussion:
Types of fracture:  Figure obtained from jaaos.org; Patellar Fractures in Adults; AAOS April 2011 vol. 19 no. 4 198-207,Figure 4 A) Nondisplaced B) Transverse C) Pole or sleeve (upper or lower) D) Comminuted nondisplaced E) Comminuted displaced F) Vertical G) Osteochondral Evaluate with physical examination first Severe knee pain and soft tissue swelling should raise suspicion for injury Concerning findings:
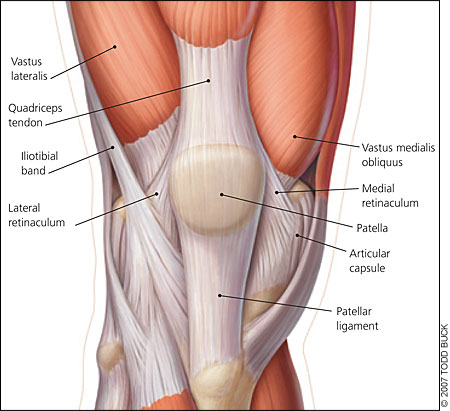 Image obtained from aafp.org, Am Fam Physician. 2007 Jan 15;75(2):194-202. Obtain Radiographs
Fracture displacement best viewed on lateral films, but obtain AP/Lat/Oblique/Sunrise to fully evaluate Degree of displacement = degree of retinacular disruption Treatment: Nonoperative:
Early active ROM with hinged knee brace after 2-3 weeks Operative:
Pearls: Watch out for patella sleeve fractures in peds – need high index of suspicion to diagnose
Bipartite patella = failure of bony fusion
Any lacerations present must be assumed to communicate with the knee joint until this assumption is disproved by a saline load joint challenge A patellar fracture is problematic and requires intervention if extensor mechanism of knee is nonfunctional = unable to perform straight leg raise test HPI:
Pre-teen male with no PMH presents to the ED after a dog bite the night before. Patient was bit on the palm of his left hand by a relative’s pit bull known to be fully vaccinated. Wound had been becoming more painful and 3rd digit is more swollen, painful, and difficult to range. No other injuries or complaints. Physical Exam: Two sub-centimeter puncture wounds to the center of the palm of the left hand, hemostatic with small amount of surrounding erythema present. 3rd digit with fusiform soft tissue swelling, increased warmth, and significant tenderness to palpation. Finger in slightly flexed positioning. Decreased ROM of the 3rd digit with flexion and significant pain with passive extension. Sensation intact to light touch throughout digits and hand. No other erythema, swelling, or significant tenderness present over LUE. 2+ palpable radial and ulnar pulses present. Radiology: No fracture or acute changes. No foreign body present. Management: Patient was admitted and was started on IV antibiotics for suspected pyogenic flexor tenosynovitis. Wound was rechecked in the morning with minimal improvement in symptoms and patient underwent I&D of digit and hand with continued IV antibiotics. Discussion: Pyogenic flexor tenosynovitis = infection of synovial sheath surrounding the flexor tendon
Pain/swelling usually delayed 24-48 hours, usually localized to the palmar aspect of one digit of the hand Kanavel signs – key physical exam findings for diagnosis
Obtain x-rays to rule out bony involvement or foreign body MRI can help diagnose but is expensive and generally unnecessary since clinical exam usually is sufficient Treatment: If early presentation:
If late presentation or if no improvement after 24 hours of conservative treatment:
Empiric Abx to consider: Otherwise healthy individuals--
Consider with dog bites-- most are polymicrobial:
Key Points: History and physical examination is key to diagnosis Start antibiotics early Consider surgical intervention when there is:
o flexor tendon sheath o deep spaces of the palm o joint spaces Kanavel signs may not be seen if patient has:
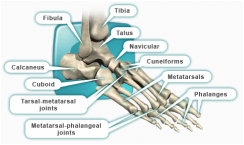
HPI: The patient is a middle-aged male with PMH of diabetes and hyperlipidemia who presented to the emergency department with right second toe pain. Two months prior, the patient dropped a heavy object on his toe causing the nail to fall off. Since that time, he has had persistent pain in that digit. Seven days prior admission, the patient reports that his second right digit turned black with associated right foot swelling and erythema. Patient denied any systemic symptoms. PE: Right second toe is black and entirely discolored with obvious necrosis. Minimal peeling at the plantar surface, 2+ DP and PT pulses bilaterally. Decreased sensation over the 2nd right toe. Patient is able to flex and extend all digits without difficulty. Mild erythema over the dorsum of the foot.  Imaging: Right foot xray: Peripheral calcified vasculopathy concerning for ischemic change. Negative for tissue pneumatosis. Negative for stress fracture. Mild degenerative arthrosis of the talonavicular joint. CTA Pelvis with unilateral runoff: Diffuse scattered atherosclerotic and intimal thickening changes within the patient's right lower extremity. Runoff from the superficial femoral artery to the level the popliteal artery. There is severe diffuse atherosclerotic change of the posterior tibial artery extending to the plantar aspect of the foot and also to the vessels supplying the digits.  Management:
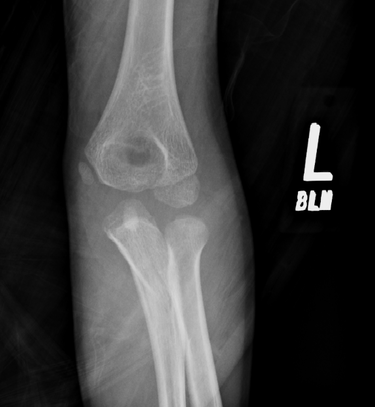
Patient received IV antibiotics in the ED given the erythema over the plantar surface of the foot. Patient admitted to orthopedic service and underwent amputation of 2nd digit. Discussion: -Gangrene is the progressive death of tissue secondary to lack of blood supply -Two most common types are dry and wet -Dry gangrene is secondary to lack of blood supply. Wet occurs when tissue becomes infected with bacteria. -Patients are increased risk because of conditions such as diabetes, trauma, smoking, obesity, excessive alcohol use and IV drug use -Symptoms include pain, shedding of skin, foul smell and skin color changes. Systemic symptoms include fever, chills, confusion, nausea, vomiting, diarrhea, and hypotension -Diagnosis includes basic laboratory work-up, xray of the affected area, CTA as needed -Treatment includes IV antibiotics to treat any overlying infection, supportive care including fluids and pain control, surgical debridement, revascularization if possible, hyperbaric oxygen and amputation if all else fails Key Points: -Initiate antibiotics early if infection is suspected -If ischemia is detected early, revascularization with vascular surgery consultation is recommended -Dry gangrene is a result of chronic ischemia -Once gangrene has developed, affected tissue is typically not salvageable and orthopedics or vascular surgery should be consulted by amputation -Gas gangrene is caused by exotoxin producing bacteria and should always be on an emergency physicians differential – ALWAYS consider this on the differential HPI: Young male otherwise healthy presenting today status post fall. Right hand dominant. Patient fell awkwardly with his arm slightly outstretched backwards off a trampoline and landed with his left arm under him. Patient had isolated pain at his left elbow. Ambulatory. No head injury or LOC. Physical Exam: Mild swelling present at the left elbow region with tenderness at the olecranon. Patient had limited range of motion at the elbow secondary to pain. Radial pulses strong and equal bilaterally. Able to give thumbs up, cross fingers, and make okay signs bilaterally. No neurologic deficits in median, radial or ulnar nerve distributions. Radiograph:
Management:
HPI:
33 year old with no prior PMH presents to the ED with left knee pain Physical Exam: Swelling over the left knee. Limited range of motion secondary to pain. No overlying laceration or abrasion. Knee is warm to the touch. Overlying cellulitis on the lateral left knee. Palpable DP and PT pulses with intact sensation in the SP, DP and tibial nerve distributions. Radiology: Normal knee Management: Patient underwent arthrocentesis. Joint fluid analysis showed only 81 cells. Presentation consistent with cellulitis and patient improved with IV antibiotics. Discussion: -Most commonly affected joints in descending order: knee, hip, elbow, ankle, sternoclavicular joint -Joints become infected by 1) bacteremia, 2) direct inoculation 3) contiguous spread from adjacent osteomyelitis -Why does it matter? It causes irreversible cartilage destruction in the joint -Involved joint is tender, warm and erythematous -WBC count, ESR and CRP aid in the diagnosis -Diagnosis is by joint fluid analysis – TAP THE JOINT! -Treatment includes early antibiotic treatment and operative irrigation and drainage of the joint Key Points: -Always think of this diagnosis when a patient presents with a tender, warm and erythematous joint -Diagnosis is by joint fluid analysis – TAP THE JOINT! -THIS IS AN ORTHOPEDIC SURGICAL EMERGENCY – Involve consultants early! |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|




 RSS Feed
RSS Feed
