 Case 1 - Lower extremity weakness
> Stanford classification - A involves the aortic root, B is limited to the descending aorta > Prsenting sx of type B dissections- chest or back pain, abrupt onset of pain > Imaging - CXR - 56,5% are nl, TTE - usef for aortic root, CT best sensitivity and specificity Therapy
Case 2 - Fatigue - dyspnea
b. Admitted to hospital - heparin drip stopped and echo gotten - shows right heart strain c. CTA showed massive Bilateral PEs Predictors of Complications from PE
Submassive PE - Rigth ventricle with dilitation and systolic dysfunction, CT - RV dysfunction, elevated BNP or troponin
0 Comments
 Dr. Zahn - The Zahn-inator Dr. Zahn - The Zahn-inator CASE 1 - Pupura, Diffuse Lymphadenopathy, Fatigue, Arthralgia, 20lb weight Loss. DDx: HUGE and includes: HIV/AIDs, syphilis, tick borne disease, endocarditis, meningococcemia, thrombocytopenia Core Concept: LUPUS
CASE 2 - 55yo with n/v/d after eating fast food. Hx of previous CVA, TIAs, and Mitral Valve Repair. Is this Acute Gastroenteritis? Nope - Imaging: right vertebral artery occlusion with posterior CVA. Core Concepts: Posterior CVA
CASE 3 - Teenager with complains of persistent shoulder pain, Normal x-rays, Tachycardic. Later found to have Hypoxia!
Initially he looked well... then he didn't. Found to have CA-MRSA subperiosteal abscess. Core Concepts - CA-MRSA
 Dr. Allen Dr. Allen Definition:
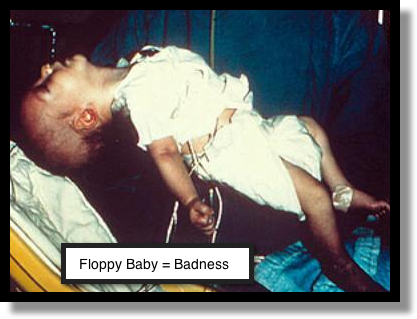 Infantile Botulism Infantile Botulism
|
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
