 **Kids... look great until they plummet. Appear well until very close to decompensation.
INTUBATION - DO IT BEFORE IT IS TOO LATE **Intubate early for children who are doing poorly, do not wait until they are becoming increasingly hypoxic and bradycardic! **40% of infant cardiac output goes to work of breathing - tremendous metabolic requirement. May need to intubate for non-respiratory reasons - use blood gases **Consider ketamine for sick neonate needing intubation/sedation INTUBATE THE STOMACH TOO!! **Decompress belly if needed: Infant diaphragm more horizontal, does not help with breathing as much. Distended gassy abdomen will severely inhibit breathing. Use NG TUBE RESUSCITATE!! GIVE FLUIDS FAST!! **FLUIDS: use up to 60cc/kg, one little bolus of 20cc/kg often gross under resuscitation. 60cc/kg is not the maximum... its the start DON'T FORGET THE SUGAR!! **Blood sugar: In infant it can drop from normal to low quickly. Can have wide range of symptoms or be asymptomatic. **sugar problems: infant brain uses 90% of glucose, head to body ratio MUCH higher in infant. Healthy infant uses 6-8 mg/kg/min sugar as opposed to 2mg/kg/min in adult **Sugar: High, keep checking. Normal, start basal rate. Low, give bolus! GET ACCESS NOW!! **IO: Difficult in infant, but it is DIFFICULT in the very young. We often wait too long to go to IO. Don't!
0 Comments
 CMCEDMasters Master CMCEDMasters Master Acquired Long QT
Bad Trauma Airway (Cricothyroidotomy, Traumatic Brain Injury
Occult Hip Fracture
 All that and then some... All that and then some... Lip and facial swelling - Angioedema to the Max!
Our New Scope is found in Room 1 of pixis- "endoscopy storz'. Attached to cmac to black plug,  29 yo bilateral leg pain Lactic acidosis
1. Resusucitate/supportive care 2. Identify cause with appropriate lab ordering 3. Empirically give Thiamine 500mg IV 4. Consider empiric Fomepizole after tox consult 5. Sodium Bicarbonate is controversial 6. When in doubt, call nephrology and dialyze Alcoholic KetoAcidosis -- Heavy etoh use with a recent binge, sudden cessation with abd pain, N/V. GI symptoms seen in 80%. -- Present with Absent ETOH level and Anion Gap metabolic acidosis. -- Due to increased betahydroxybutyrate ketone body, UA does not pick up ketone bodies on dip. -- Rarely will see severe lactic acidosis and if present think sepsis, seizures or thiamine deficiency. Tx:
Thiamine deficiency Pyruvate cannot enter TCA cycle causing high lactic acidosis resulting in Dry (neurologic) and Wet (cardiac) Beriberi. Also causes Wernicke (triad of AMS, opthalmoplegia, and ataxia seen only in 10% of patients). At risk- etoh, iatrogenic, aids, malignancy, gastric bypass, TPN 44yo fall from standing

Congenital Adrenal Hyperplasia
Always consider adrenal insufficiency in hypotensive patients who remain hypotensive despite appropriate fluid resuscitation and initiation of pressors (whether adult or pediatric)... but particularly think of it in neonates!!
2) Age-based - 0-3 yo: 25mg IV; 3-12 yo: 50mg IV; >12 yo: 100mg IV 3) Randy's Rules (from the brilliant mind of Dr. Cordle) - Give at LEAST 25mg; 3x their current dose; or 2mg/kg 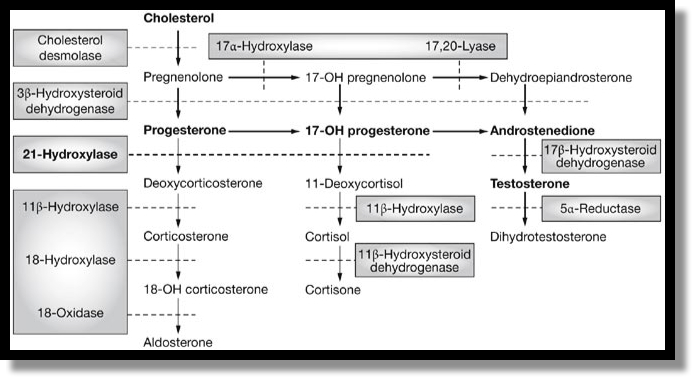 Steroid Production
23 yo with Headache --- and she's Pregnant PreEclampsia
Catecholamine-Secreting Tumors
Swollen Leg Phlegmasia
|
Archives
August 2018
Categories
All
|

 RSS Feed
RSS Feed
