|
HPI: Otherwise healthy middle-aged male presents to ED with L arm pain. He fell backwards off a ladder at work bracing the fall with his outstretched L hand. There was immediate pain/swelling to the elbow with inability to range the joint. He denies other injuries, and all vital signs are within normal limits. Exam: L arm adducted w/ elbow held in flexed position. Obvious swelling about elbow joint with prominent olecranon and shortened forearm. Compartments soft, distal motor/sensory function is intact. 2+ radial/ulnar pulses with cap refill <2 seconds. (x-ray shown below) 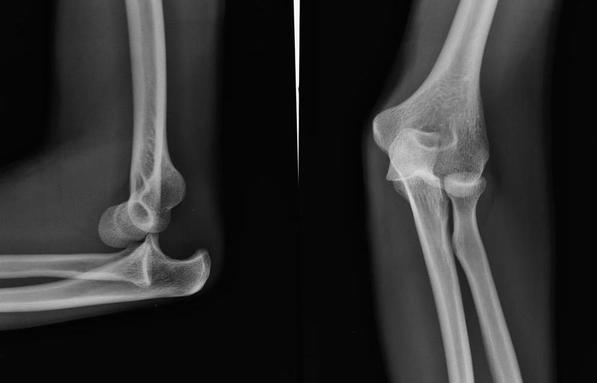 Discussion: Elbow dislocation is the second most common major joint dislocation seen in the ED (behind the shoulder). 80% of elbow dislocations are posterolateral and occur as a combination of: 1) axial loading, 2) forearm supination/external rotation, and 3) posterolateral valgus force to the elbow. · Simple dislocation - no associated fracture (approx 50-60% of cases). · Complex dislocation - one or multiple associated fractures present. Indications for Operative Repair include: 1) complex dislocation, 2) chronic dislocation, or 3) persistently unstable dislocation following attempted reduction. However, acute simple dislocation can typically be treated Non-Operatively w/ closed reduction and splinting. Multiple techniques for reduction exist: Reduction Technique #1 Prone position w/ elbow flexed at 90 degrees and humerus supported by the edge of the stretcher. Apply downward traction to patient’s forearm held in slight pronation, while using your other hand to apply downward and/or medial pressure to the olecranon.  Reduction Technique #2 Supine or seated position w/ elbow held in slight flexion. Perform inline traction while supinating the forearm, with a second provider giving countertraction to the humerus if necessary. Gentle flexion of the elbow and/or medial pressure on the olecranon may be necessary to reduce lateral dislocations.  (YouTube video for demonstration: https://www.youtube.com/watch?v=mlAOGgocRnk)
After successful reduction, perform gentle ROM testing. Inability to range the joint smoothly raises suspicion for fracture, unsuccessful reduction, or re-dislocation. Full elbow extension is not necessary, as the joint is often still unstable in fully extended position. Place a posterior splint w/ forearm in slight pronation and elbow flexed at 90 degrees. Obtain post-reduction films, ensure soft compartments, and confirm intact neurovascular status. Orthopedic follow-up in 7-10 days. Obtain immediate orthopedic consultation for neurovascular compromise, fracture, or reduction failure. Management Pearls: · Plain films to diagnose dislocation and/or need for operative repair · Analgesia/anxiolysis (IV narcotics, hematoma block, +/- procedural sedation) · Successful reduction, gentle ROM, post-reduction films · Confirm intact neurovascular status · Posterior splint, immobilize 7-10 days, f/u with Orthopedics as outpatient By Dr. Blake Johnson References: 1. Aiyer A, Moore D. “Elbow Dislocation” [Web log post]. Retrieved 10 Sept 2015, from http://www.orthobullets.com/trauma/1018/elbow-dislocation. 2. Halstead, M. “Elbow Dislocation.” eMedicine/Medscape, 5 Aug 2014. Web. Retrieved 10 Sept 2015, from http://emedicine.medscape.com/article/96758-overview. 3. Case courtesy of Dr Maulik S Patel, Radiopaedia.org, rID: 14118. http://radiopaedia.org/articles/elbow-dislocation (image 1) 4. Video courtesy of Dr. Fakhouri, MidAmerica Orthopaedics and MidAmerica Hand To Shoulder Clinic. “Posterior Elbow Dislocation & Reduction.” https://www.youtube.com/watch?v=mlAOGgocRnk. 5. http://emedicine.medscape.com/article/96758-workup#c7 (image 2) 6. http://lifeinthefastlane.com/elbow-dislocation/ (image 3)
0 Comments
HPI: Middle-aged male with no medical history presents to the ED with a laceration to his left middle fingertip. He was using a circular saw to cut wood this afternoon when he inadvertently cut his left middle finger. He denies other injuries, and all vital signs are within normal limits. Exam: Deep laceration to dorsal surface of distal phalanx on L middle finger involving the lateral nail bed. Full motor/sensory function is intact. Cap refill <2 seconds. Plain films negative for acute fracture/dislocation. (representative image seen below)  Discussion: Fingertip injuries are the most common hand injuries seen in the ED, and evidence shows effective early treatment clearly results in best cosmetic and functional outcomes. Special consideration is taken when injury involves the nail bed. · Germinal Matrix - soft tissue at base of the nail responsible for nail generation/growth. · Sterile Matrix - soft tissue adherent to underside of the nail plate responsible for nail strength/thickness. If nail plate is avulsed or subungual hematoma involves >50% of nail bed, then nail should be removed for hematoma evacuation/irrigation. If underlying laceration involves the germinal or sterile matrix, it should be repaired w/ 6-0 absorbable suture or Dermabond. Soak nail plate in a povidone iodine solution while performing repair. Replace the extracted nail plate at completion to splint the eponychial folds and better mold the edges of the repair for optimal healing (can be sutured in place). Apply a nonadherent dressing and consider a splint to immobilize DIP joint and protect the fingertip. 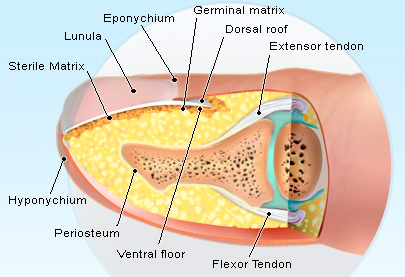 Management Pearls:
· Pain control (digital block), update tetanus status, Abx prophylaxis · Plain films to rule-out distal phalanx fracture · Copious irrigation and close inspection of wound · Nail plate removal and/or nail bed repair as indicated · Replace nail plate to splint eponychial fold and promote nail growth at germinal matrix · Non-urgent orthopedic follow-up as outpatient By Dr. Blake Johnson References: 1. Jones, T. Nail Bed Injury [Web log post]. Retrieved 3 Sept 2015, from http://www.orthobullets.com/hand/6109/nail-bed-injury. 2. Strauss EJ, Weil WM, Jordan C, et al. A prospective, randomized, controlled trial of 2-octylcyanoacrylate versus suture repair for nail bed injuries. J Hand Surg [Am]. 2008 Feb. 33(2):250-3. 3. Yallapragada, R. “Nail Bed Laceration Repair.” eMedicine/Medscape, 25 June 2015. Web. Retrieved 3 Sept 2015, from http://emedicine.medscape.com/article/80792-overview. 4. http://www.sawaccidents.com/table-saw-injury-pictures.htm (image 1) 5. http://www.medicinenet.com/image-collection/fingernail_anatomy_picture/picture.htm (image 2) HPI: 18 yo male involved in a head on MVC. Patient was the unrestrained driver. The patient was initially unconscious but is now combative. Per EMS there is an obvious deformity to the right lower leg with “bone sticking out.” Patient is slightly tachycardic on arrival with a HR of 102 with a blood pressure of 132/90 and has a GCS of 15. EXAM: The primary survey is unremarkable and the patient continues to maintain stable vital signs. During the secondary survey a 3 cm laceration with what appears to be protruding bone is noted 20 cm distal to the R knee. Patient has intact sensation distal to the injury with strong DP and PT pulses with good capillary refill. Steady dark bleeding is noted from the wound. The motor exam is limited by pain and uncooperative patient. IMAGING:  MANAGEMENT: 1. First priority is trauma resuscitation 2. Thorough neurovascular examination 3. Irrigation and debridement of the site 4. Application of a splint to the affected limb for temporary stabilization 5. In addition to standard trauma resuscitation tetanus prophylaxis and early administration of antibiotics is indicated
DISCUSSION: - Patients will need operative debridement and fixation of their fractures - Copious irrigation in the OR is key for preventing infection - Direct pressure, NOT blind clamping is the best way to control bleeding - Open fractures can often wait until the following day for operative repair. At one time it was thought every open fracture required operative repair within 6 hours to lower the risk of infection. This is NOT true. KEY POINTS: - Tetanus and early antibiotic administration a MUST.
- Thorough neurovascular examination prior to splinting - Remove gross debris from fracture site and cover with moist gauze. - Does not require immediate operative repair - Apply temporary splint to stabilize fracture HPI: 27 yo male playing basketball “jammed” his right ring finger which was immediately followed by pain, shortening of the digit and inability to flex his finger. Exam: Obvious deformity at the right ring finger PIP joint with associated ecchymosis. Sensation to light touch intact and good capillary refill at the affected finger. Patient unable to flex at affected digit. No other identifiable injuries noted. Images:
 Discussion:
Management:
Key Points:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696003/
Orthobullets.com HPI: 35 yo male construction worker falls from 15 feet off of a ladder complaining of severe R foot/ankle pain as well as lower back pain. Exam: Obvious swelling and ecchymosis of the R ankle and heel with associated tenderness. No deformity or tenderness to the L foot/ankle. Midline lumbar tenderness. Patient has palpable PT/DP pulses bilaterally with no noted sensory deficits. Images: Tongue type:  (Credits: South Florida Institute of Sports Medicine) Bohler’s angle (normal):  Bohler’s angle (reduced):  (Radiopedia.org) Management:
#Initial ED - Obtain AP, Lateral, oblique foot plain film images at minimum. - Often Broden, Harris views will be requested for complete visualization. #Non-operative - Extra-articular fractures with minimal displacement and intact Achilles tendon. - Sanders Type I fractures - Bulky cast with extra padding around the heel and ankle. - Requires EXTENDED non-weightbearing status. Often approaches 12 weeks. - All require referral to orthopedic surgery #Operative - Prompt recognition of Tongue-type fractures as illustrated above. - Orthopedic EMERGENCY as skin overlying the fracture has a high instance of compromised vascularity and death/necrosis. - Displaced intraarticular fractures - Sanders type II-IV Discussion: - Common in males aged 35-45, often work related - Due to extended non-weightbearing requirement these injuries have large socioeconomic impact on patients - High complication rate if not recognised early - Contralateral calcaneus and spine have a 10% concomitant injury rate. - Look for reduced Bohler angle and increased angle of Gissane Key Points: - Be vigilant as secondary injuries very common - Most commonly the spine and contralateral calcaneus - Recognise tongue-type fractures early and prompt notification of orthopedic surgery - Don’t forget the spine in axial load type injuries References: http://www.orthobullets.com/trauma/1051/calcaneus-fractures HPI: Approximately 5 y/o male presents with right elbow pain and refusal to move the right arm after falling from a chair on an outstretched arm. EXAM: Gross deformity present on the distal humerus, just proximal to the elbow with mild skin tenting and tenderness. Refusal to move the elbow joint. Unable to extend the wrist and digits. Remainder of exam normal. IMAGES: Obtain AP and lateral elbow views  Normal Elbow: anterior humerus line intersects the middle third of the capitellum Gartland Classifications: 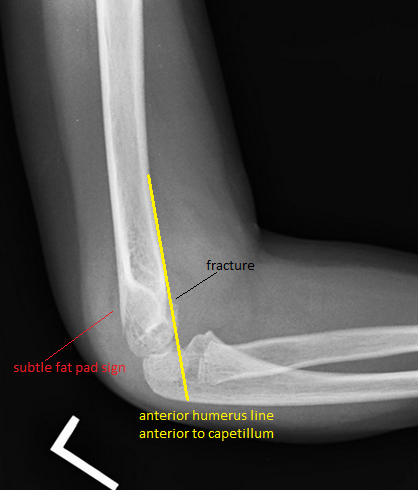 Garland Type 1: Non-displaced  Garland Type II: Displaced with posterior cortex intact  Garland Type III: Completely displaced
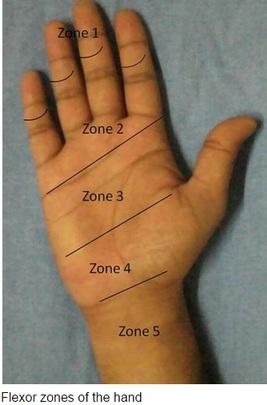
MANAGEMENT: #Non-operative - Posterior long arm splint with less than 90 degrees of flexion - Type I and some Type II fractures. - Consult Ortho for Type II fractures to determine if operative management is needed #Operative - All Type III fractures, some Type II fractures - “floating elbow” : ipsilateral supracondylar and forearm fractures - Immediate operative management if vascular compromise is present - Reduce in ER if any vascular compromise is present - Most are admissions with next day operative fixation DISCUSSION: - Incredibly common in 5-7 year olds with a fall on an outstretched arm. - Radial, ulnar, anterior interosseous nerve neurapraxia all very common and resolve with reduction without long term effects but require expedited management - Very easy to miss a type I fracture, use the anterior humerus line and fat pad sign - Garland classification above, determines management - Can be associated with vascular injury (~1%), this requires immediate reduction KEY POINTS: - Use the anterior humerus line and fat pad sign to help find subtle fractures - High suspicion in any fall on an outstretched arm - Remember the Garland Classifications - Most Type II and all Type III will require operative management and admission - A posterior long arm splint for Type I fractures - Always assess for neurovascular compromise By Dr. Mohamed El-Kara HPI: Approximately 30 y/o right handed male presents with a laceration to base of the left thumb and inability to move his thumb. EXAM: Left hand: Laceration extends along the volar base of the thumb, no other injuries noted. Thumb is held in extension with limited opposition of the thumb. Complete inability to flex the thumb at the ITP. Ability to extend the thumb is preserved. When the wrist is extended, the thumb remains in extension. Decreased two point discrimination distal to the laceration. Ability to cross 2nd and 3rd digits is preserved. Remainder of sensation and motor function of the digits is intact. IMAGES: X-rays are needed only if underlying fracture is suspected (malalignment of digits)
 MANAGEMENT
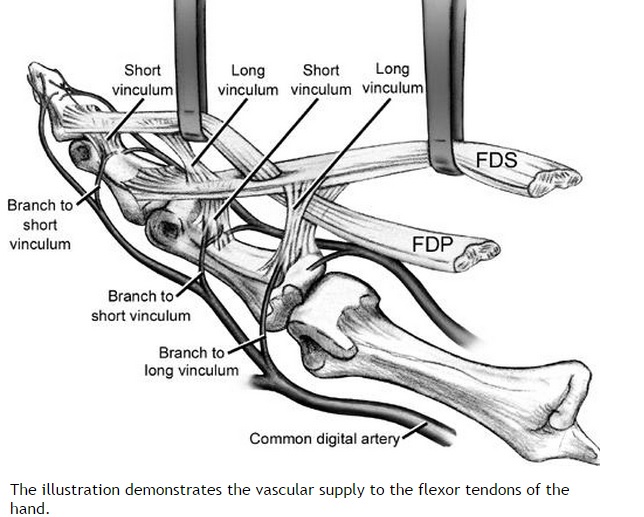
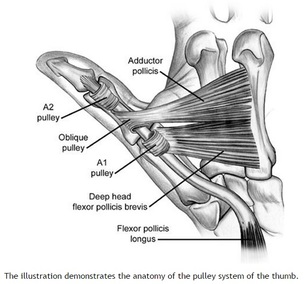
#ED Management - Assessment for other injuries - Thorough irrigation of wound and closure of skin - Splint in slight flexion - One dose of Ancef preferred - Very close follow up with hand specialist (1-3 days) #Non-Operative - <60% of tendon width affected - Wound care and hand rehab #Operative - >60% of tendon width affected - Ideally within 2 weeks of injury - Extensive hand rehab starting immediately after repair - Lots of repair techniques available depending on zone of injury. Outside the scope of this post DISCUSSION - This patient had a complete FPL transection. Laceration repaired, given 2 day f/u. - Flexor tendons need to be fixed ASAP but not emergently - More urgency than extensor tendon repairs - High suspicion with any volar laceration - Outcomes very variable depending on zone of injury and time until surgery - Hand rehabilitation is paramount to prevent scarring and loss of function - FDP inserts in the DIP. FDS inserts in the PIP. - High probability of concomitant neurovascular injury, associated with worse outcomes - Tenodesis effect - naturally, the digits flex when the wrist is extended. If abnormal very high likelihood of flexor tendon injury. KEY POINTS - High suspicion with volar lacerations and digits in extension - Remember the tenodesis effect - Always check for neurovascular injury - Higher urgency than extensor tendon injuries - Urgent but not emergent surgery required - Can close in the ED and arrange very close hand follow up - Splint in flexion - Be aware of the different different zones of the hand but extensive detail not needed. by Dr. Mohamed El-Kara REFERENCES: http://www.orthobullets.com/hand/6031/flexor-tendon-injuries HPI: 55 y/o male with history of etoh abuse and bilateral THA presents with left hip pain and inability to walk. He has been drinking etoh and playing with his grandchildren when he noticed his left hip dislocated. This occurs monthly. EXAM: Left leg is slightly shorter than right. Leg and hip in flexion, adduction, and internal rotation. Able to palpate the femoral head. No deficits of foot function noted. IMAGES: Obtain AP and Lateral Hip  MANAGEMENT:
#Non-operative - First line when no associated fractures are present - Frequently requires sedation but not paralyzation (unlike traumatic which requires both) - Flex the hip and knee to 90 degrees, place axial traction, internally rotate the hip with a second person placing counter traction on the hip - Second person can help guide the femoral head into proper positioning - Place in knee immobilizer post reduction to prevent recurrence #Operative - Indications include inability to reduce non-operatively, associated fractures, multiple dislocations - Revision of THA can occur as an outpatient and does not require admission DISCUSSION: - Posterior dislocation occurs in 75-90% of cases - Risk factors: prior hips surgery, etoh abuse, age >70, malpositioning of components, etoh abuse, neuromuscular disease - Mechanism: hip flexion, adduction with internal rotation. (ie: shoe tying, sitting on toilet) - Easier to reduce than traumatic dislocations, should not require paralytics - Fracture of the femur is a complication of the procedure, especially with predisposing diseases (etoh abuse, chronic steroids) - AT CMC, protocol is to reduce in PACU under sedation - Can d/c home following reduction with ortho follow up - Anterior dislocations can be reduced with axial traction and internal rotation without flexion of the hip. KEY POINTS: - 90% posterior dislocations (hip in flexion, adduction, internal rotation) - Hip x-rays to assess for dislocation type and for fractures - Frequently only requires sedation without paralytics - Reduction by hip/knee flexion to 90 degrees, axial traction and internal rotation - Frequently requires a lot of force to reduce - Place in knee immobilizer post reduction to prevent recurrence - Don’t break the femur by Dr. Mohamed El-Kara References: http://medapparatus.com/Ortho/Images/JointArthroplasty/DislocatedLeftHipArthroplasty.jpg http://www.orthobullets.com/recon/5012/tha-dislocation HPI: 5 year old female presents with right arm pain after falling on a chair. Her arm was pinned in between the chair and the floor. She had immediate pain but it resolved. The following day she has increased pain and swelling in the right arm. EXAM: Swelling is noted in the proximal forearm. Tenderness to palpation present on the proximal ulna as well as radial head. No tenderness to the medial condyle, lateral condyle, or olecranon. Passive and active range of motion of the elbow is full but painful. No motor or sensory deficits of the hand. IMAGING. AP and lateral views of the elbow.   Note there is plastic deformation of the ulna without a complete fracture
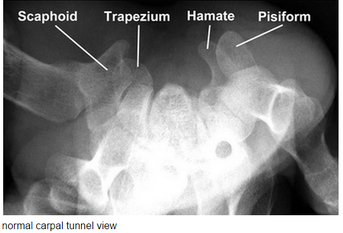
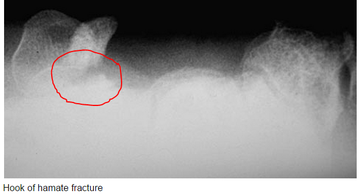
Always assess the radial head, it should point towards the capitulum MANAGEMENT #Non-operative - Closed reduction of ulna and radial head dislocation and long arm casting - If no ortho available, attempt to reduce radial head and place in a posterior splint. - Axial traction traction to restore ulnar length - Need to successfully reduce radial head dislocation as well - Immobilize in 110 degrees flexion and full supination. #Operative - Indicated if radial head or ulnar length are unstable following reduction - Indicated in Bado Type IV fractures (complete fx of Ulna and Radius) - Frequently required in missed diagnosis. DISCUSSION - A Monteggia fracture is radial head dislocation plus a proximal ulna fracture or plastic deformation of the ulna - Peak age range 4-10 years, fall onto pronated arm.. - Frequently missed since the ulna may only have plastic deformation, have a high suspicion if there is pain over the radial head or evidence of radial head dislocation. - Complications include posterior interosseous nerve neurapraxia (finger drop, radial wrist deviation). - Loss of forearm motion with delayed treatment (2-3 weeks) - Different classifications are present (Bado) but not as key as recognizing the fracture. - This patient was casted and follow up arranged. KEY POINTS - Have a high index of suspicion when there is radial head tenderness or dislocation - Ulna may show only plastic deformation - Radial head should always point towards the capitulum - Obtain contralateral arm films if comparison is needed. - ED management without ortho includes reduction with posterior splint placement. Close f/u. - Majority of cases result in non-operative management. - Frequently missed By Dr. Mohamed El-Kara REFERENCES http://www.orthobullets.com/pediatrics/4015/monteggia-fracture--pediatric http://emedicine.medscape.com/article/415822-overview#a5 HPI: Young adult presents with distal left 5th digit discoloration after a sporting event. He felt intermittent sharp pain in the ulnar portion of his left hand but otherwise no other complaints immediately following the injury. The following day, he had discoloration of his left 5th digit but the pain resolved. EXAM: Purplish discoloration present in the left 5th digit distal to the DIP. Allen’s test reveals reduced ulnar blood flow. No pain to palpation of any portion of the hand. Flexion/extension intact in all left hand joints. 2 point discrimination reduced in the left 5th digit. Doppler flow present in the superficial blood vessels. IMAGING: Best seen with a carpal tunnel view. Also obtain an AP view.
MANAGEMENT:
Non-operative - Acute hook or body fractures - 6 weeks immobilization Operative - Excision of hamate fracture fragment - Chronic hook of hamate with non-union - neurovascular compromise - ORIF with very little benefit DISCUSSION/PEARLS: - This was most likely a chronic fracture with resulting non-union and was reinjured. - Surgical findings included engorged veins and arteries - Associated with golf and baseball injuries - Usual presentation: Hypothenar pain to palpation - Pain with tight grip and decreased grip strength - In Chronic cases: Ulnar nerve compression resulting in 4th, 5th digit paresthesias - Rarely: Ulnar artery thrombosis KEY POINTS - Consider with ulnar sided hand pain with golf and baseball injuries - Pain with grip strength - Obtain a carpal tunnel view - Hamate body fracture very rare, hook fracture much more common - Non-union results in chronic ulnar nerve symptoms - Non-operative management is appropriate if acute without any neurovascular compromise - Operative management involves excision of fractured portion. By Dr. Mohammad El Kara REFERENCES: http://openi.nlm.nih.gov/detailedresult.php?img=2904904_256_2009_842_Fig1_HTML&query=null&req=4&npos=-1 http://www.orthobullets.com/hand/6035/hook-of-hamate-fracture |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed

{kind=link}