|
PEM Fellows Journal Watch Quarterly
Your Up-to-date summaries of relevant pediatric emergency medicine literature from the comfort of your home Editor – Jeremiah Smith Columnists Christyn Magill JR Young Kat Bryant Simone Lawson All Articles are archived @ http://www.cmcedmasters.com/pem-journal-watch.html December January Synopsis – This study compared career preparation and potential attrition of the PEM workforce with a prior assessment done in 1998. This was performed via an email sent to members of the AAP SOME and non-AAP members board certified in PEM. 2,120 surveys were sent and 895 individuals responded (40.8%). 53.7% were female which was up from 44% in 1998. 62.9% practiced in a free-standing children’s hospital and 60% of their time was spent in direct patient care. Nearly 50% spent time in research and 50% performed other activities like EMS, disaster medicine, child abuse, etc. 21.3% had dedicated time for quality/safety. 95.6% felt fellowship prepared them well for clinical care but felt less prepared for research (49.2%) and administration (38.7%). 46% plan to change to clinical activity within 5 years. 88.5% of respondents reported feelings of burn out at work or callousness toward people as a result of work (67.5%) at least monthly. 1 in 5 reported these feelings weekly. They concluded that many were satisfied with fellowship preparation for professional activities but there are gaps remaining in training for nonclinical activities. They also felt that burnout is prevalent and there is likely to be substantial attrition of PEM providers in the near future. Gorelick M, Schremmer R, Ruch-Ross H, et al. Current Workforce Characteristics and Burnout in Pediatric Emergency Medicine. Acad Emerg Med 2016;23:48-54 Synopsis - Acute pain is commonly under treated in children. Studies have also shown in adults disparities in analgesia in different races and ethnicities. This study in Israel assessed if there were disparities between Arabic and Jewish children for opioid analgesia for acute pain, specifically in fractures and dislocations. Over a 4 year period this retrospective cohort study collected pain assessments and opioid analgesia given by Jewish nurses to both Jewish and Arabic children. This study found no difference in treatment in the two groups, suggesting ethnicity has no effect on opioid analgesia in acute pain in this pediatric ED. Shavit I, Brumer E, Shavit D, et al. Emergency Department Pain Management in Pediatric Patients with Fracture or Dislocation in a Bi-Ethnic Population. Ann Emerg Med 2016;67:e1 9-14 Synopsis: This study reviewed Poison Control Center data over a 10-year period to characterize the epidemiology of drug exposures amongst children 0-6 months of age, with the goal of therefore offering better preventative strategies based on presentation characteristics. Results indicate that unintentional drug exposures are common, and the majority of exposures are clinically benign. The PCC network is vastly underutilized, thereby increasing direct presentation to the ED. Improved anticipatory guidance is recommended, but what other strategies should we consider to prevent inappropriate ED referrals? An Evidence-Based Approach to Minimizing Acute Procedural Pain in the Emergency Department and Beyond. Samina A, McGrath T, Drendel A. An Evidence-Based Approach to Minimizing Acute Procedural Pain in the Emergency Department and Beyond. Ped Emerg Care 2016;32:36-42 Synopsis – This was a review article intended for emergency medical providers for children aimed at familiarizing clinicians with pediatric pulmonary hypertension. They reviewed pathophysiology, clinical presentation, initial diagnostic strategies, basic chronic management, and management of pulmonary hypertensive crisis. Del Pizzo J, Hanna B. Emergency Management of Pediatric Pulmonary Hypertension. Ped Emerg Care 2016;32:49-55 February Synopsis – As we know, nonvisualization of the appendix often presents a diagnostic dilemma in the emergency department. Their primary aim was to quantify the accuracy of MRI and US in the setting of a nonvisualized appendix. They also reported the sensitivity of MRI and US and correlation between the two imaging modalities. They retrospectively reviewed all pediatric emergency department patients aged 3-21 years who underwent a MRI (N = 205) and/or US (N= 583) for the evaluation of appendicitis. They had 589 included patients with 146 having appendicitis. If the appendix was nonvisualized with no secondary signs of appendicitis, MRI had an accuracy of 100% and US was 91.4%. If it was nonvisualized but had secondary signs of appendicitis, MRI had an accuracy of 50% and US was 38.9%. There was moderate correlation between the two (0.573). They concluded that if MRI is used but the appendix is not visualized, MRI is effective at excluding appendicitis if there are no secondary signs though less helpful if there are secondary signs of appendicitis. It appears to be somewhat more useful than a non-diagnostic US with or without secondary signs of appendicitis. In addition, 8.6% of patients with a nonvisualized appendix had appendicitis. Kearl Y, Claudius I, Behar S, et al. Accuracy of Magnetic Resonance Imaging and Ultrasound for Appendicitis in Diagnostic and Nondiagnostic Studies. Acad Emerg Med 2016;23:179-185 Synopsis - This study evaluated the retention for PALS/NRP protocols and procedures at 6wks, 18wks and 52wks after an initial training simulation session. They found that there was a predicted variable initial score/retention score for different experienced practitioners; but in all levels of experience the retention/competency scores decreased as time passed showing that retraining/refresher intervals would be helpful to maintain important PALS/NRP skills. Andreatta P, Dooley-Hash S, Klotz J, et al. Retention Curves for Pediatric and Neonatal Intubation Skills after Simulation-Based Training. Ped Emerg Care 2016;32:71-76 Synopsis – This was the results of an electronic questionnaire distributed to urgent care center administrators. An urgent care center was identified by the American Academy of Urgent Care Medicine directory. They found the most common diagnoses reported were otitis media, URI, strep pharyngitis, bronchiolitis, and extremity sprain/strain. Seventy-one percent have contacted EMS for transport of a critical ill or injured child within one year. Urgent care centers had the reported availability of the following essential medications and equipment: oxygen source (75%), nebulized inhaled β-agonist (95%), intravenous epinephrine (88%), oxygen masks/cannula (89%), bag-valve mask resuscitator (81%), suctioning device (60%), and AED (80%). Centers reported the presence of the following written emergency plans: respiratory distress (40%), seizures (67%), dehydration/shock (69%), head injury (59%), neck injury (67%), significant fracture (69%), and blunt chest or abdominal injury (81%). Only 47% performed formal case review in a QI format. Wilkinson R, Olympia R, Dunnick J, et al. Pediatric Care Provided at Urgent Care Centers in the United States: Compliance with Recommendations for Emergency Preparedness. Ped Emerg Care 2016;32:77-81 Synopsis: Pain control makes sense. The majority of papers reviewed agree with this. This paper has no METHODS section, fails to even mention the data surrounding clinical practice guidelines until the next to last paragraph, and generally speaks in broad terms without specific details. The paper relies heavily on Cochrane reviews without digging further. It suggests that clinical practice guidelines are validated to help improve overall efficacy, but the studies they reference are for neonates or post-operative pain control, not specific the pediatric patients in the ED. It appears that common sense wins out (pain control is important and humane), but that people need to utilize it – meaning that we need to remember the importance of analgesia, and therefore prioritize it, rather than think of it as an afterthought. Kang M, Brooks D. US Poison Control Center Calls for Infants 6 Months of Age and Younger. Pediatrics 2016;137:1-7 Synopsis – This statement updated previous recommendations with new evidence on the prevention, assessment, and treatment of neonatal procedural pain. This important because the prevention of pain in neonates should be the goal of all healthcare professionals tasked with their medical care. Preterm infants in the NICU are not only at the greatest risk of neurodevelopmental impairment but are also exposed to the greatest number of painful stimuli in the NICU. There is a paucity of literature regarding how to effectively and safely treat their pain. What has been proven and studied is underused for routine but painful procedures. They recommend that every health care facility caring for neonates should: implement a pain-prevention program with strategies to minimize the number of painful procedures performed and a pain assessment and management plan including both assessment, pharmacologic and non-pharmacologic, and measures to minimize pain with surgery and major procedures should be implemented. Committee on Fetus and Newborn, Section on Anesthesiology and Pain Medicine. Prevention and Management of Procedural Pain in the Neonate: An Update. Pediatrics 2016;137:1-13 March Synopsis – This is a queried report from an emergency medicine e-mail discussion list and social media allergy group to identify injuries in children as the result of epinephrine autoinjector use. Twenty-two cases were described. Twenty-one of these were during intentional use. Seventeen children experienced lacerations, four resulted in the needle being stuck in the child’s limb, and one resulted in a laceration to a nurses’ finger. In six cases the operator was a health care provider, fourteen cases by the patient’s parent, and one by the patient. They concluded that these are obviously lifesaving devices in the management of anaphylaxis but injury such as laceration can occur. Minimizing injection time, improving device design, and providing leg immobilization instructions may decrease risk of injury. Brown J, Tuuri R, Akhter S, et al. Lacerations and Embedded Needles Caused by Epinephrine Autoinjector Use in Children. Ann Emerg Med 2016;67:307-315
0 Comments
By Christyn Magill MD CC: infant vomiting HPI: 2mo term female, born at 38 weeks gestation, SVD, no complications, normal prenatal labs. Presents with 3 days of projectile vomiting about 10-15 minutes after feeds. Initially vomitus appeared to be regurgitated food. Now, vomitus is darker in color, but no bright red blood, non bilious. Decreased UOP. Normal bowel movements per parents. Normal energy. Acting hungry. Parents deny fevers, sick contacts, rashes, diarrhea. Vomiting seems to bother child and gets fussy, but acts normally in between feeds. This is a first child for the family. Physical Exam: VS: T 98.6F rectal, HR 135, BP 114/74, RR 44, O2 98% on RA GENERAL: Laughs and smiles, very active in the ED, not clinically dehydrated HEENT: PERRL, EOMI, moist mucous membranes, no icterus, TM's NL, Oral-pharynx NL, nares NL CHEST: Normal S1 and S2, no murmurs, lungs clear to auscultation ABD: Tenderness-none, no HSM, bowel sounds NL Rectal: normal tone, small amt stool in vault, Hemoccult-positive stool BACK: Non tender, no costovertebral angle tenderness EXTREMITY: Normal active full ROM throughout all extremities, no tenderness, appearance normal GU: Normal external female genitalia SKIN: No pallor/rashes, warm & moist, brisk cap refill NEURO: Good suck, grasp, makes eye contact, social smile, +Moro reflex, Gross motor normal, gross sensation intact LYMPH: No lymphadenopathy What is on your differential diagnosis? What is your highest suspicion? What studies would you do on this patient in the ED? The following studies were done: VBG: pH 7.418, PCO2 28.8, PO2 49, Lactate 2.87, HCO3 18.6, Base deficit 5 Urine dip: glu-neg, bili-neg, ketones-large (80), SG-1.030, pH 6.0, prot-1+, urobil-normal, nitrate- neg, leuk-neg CBC: WBC 13.4K, Hb 10.9, Hct 32%, Plt 430 Chem8: Na 137, K 4.8, Cl 103, CO2 18, BUN 10, Cr <0.2, Glu 90 Hepatic: TProtein 5.4, Albumin 4.0, TBili 1.2, Dbili 0.2, Alk Phos 344, ALT 24, AST 34 CRP <0.5 Imaging: 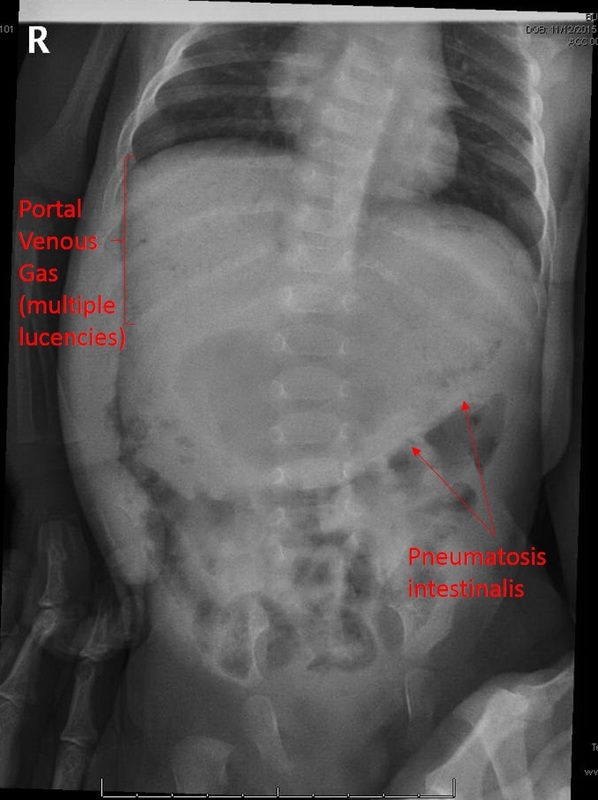 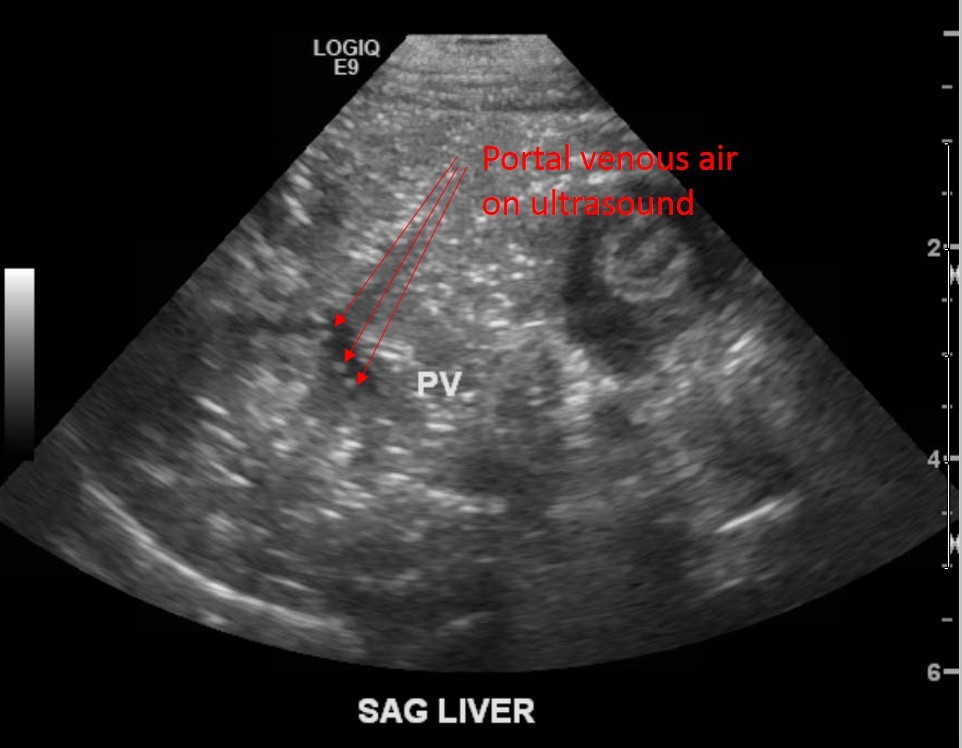 What is your diagnosis based on these studies? What is your management? Diagnosis: Necrotizing Enterocolitis Clinical Question: How do I recognize this in the emergency department, and what do I do about it? Helpful hint: http://pedemmorsels.com/necrotizing-enterocolitis/ Discussion:[1, 2]
Pathology
Epidemiology- Often, but not always, the term babies who develop NEC have some sort of underlying abnormality.[4-6]
Usually presents earlier in term babies- In one retrospective study done by Sharma et al, the extremely premature infants presented with symptoms of NEC an average of 22 days of life, whereas the term babies had symptoms an average of 3 DOL. But this is not always true, as was the case with our baby above. Symptoms/Stages Modified Bell’s Criteria From Up To Date: 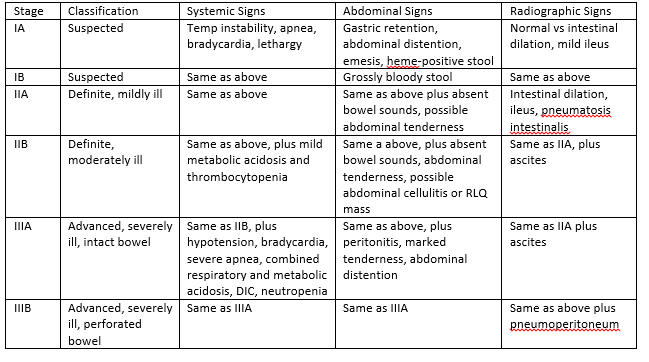 Workup[2]
CBC plus diff, BMP, LFTs (if more advanced stages), VBG Thrombocytopenia, metabolic acidosis, hyperglycemia are trended for worsening disease. Plain films- upright and lateral decubitus to eval for free air, pneumatosis intestinalis, portal venous gas. RUQ Ultrasound to show portal venous gas. [7] Treatment[8] Medical- Antibiotics, bowel rest, supportive care, lab and radiologic monitoring. Antibiotic possible regimens (from UTD): ●Ampicillin, gentamicin (or amikacin), and metronidazole ●Ampicillin, gentamicin (or amikacin), and clindamycin ●Ampicillin, cefotaxime, and metronidazole ●Piperacillin-tazobactam and gentamicin (or amikacin) ●Vancomycin, piperacillin-tazobactam, and gentamicin ●Meropenem *Vancomycin instead of Ampicillin if in high MRSA area *Add Fluconazole if worried about fungal infection Surgical[9, 10]
Complications[6, 11] Acute- sepsis, meningitis, peritonitis, abscess formation, DIC, hypotension, shock, respiratory failure, hypoglycemia, metabolic acidosis Late- intestinal stricture, short gut syndrome *intestinal strictures in 9-36%, not significantly related to medical vs surgical treatment, drain vs laparotomy, gestational age, pneumatosis intestinalis. Term infants- 3% risk of NEC, 16% mortality. Updates Probiotics are now being studied for protective potential. [5] Back to our patient:
Clinical Pearls for ED:
References: 1. Sakellaris, G., et al., Gastrointestinal perforations in neonatal period: experience over 10 years. Pediatr Emerg Care, 2012. 28(9): p. 886-8. 2. Solomkin, J.S., et al., Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis, 2010. 50(2): p. 133-64. 3. Sharma, R., et al., Impact of gestational age on the clinical presentation and surgical outcome of necrotizing enterocolitis. J Perinatol, 2006. 26(6): p. 342-7. 4. Short, S.S., et al., Late onset of necrotizing enterocolitis in the full-term infant is associated with increased mortality: results from a two-center analysis. J Pediatr Surg, 2014. 49(6): p. 950-3. 5. Terrin, G., A. Scipione, and M. De Curtis, Update in pathogenesis and prospective in treatment of necrotizing enterocolitis. Biomed Res Int, 2014. 2014: p. 543765. 6. Lambert, D.K., et al., Necrotizing enterocolitis in term neonates: data from a multihospital health-care system. J Perinatol, 2007. 27(7): p. 437-43. 7. Buonomo, C., The radiology of necrotizing enterocolitis. Radiol Clin North Am, 1999. 37(6): p. 1187-98, vii. 8. Barie, P.S., et al., A randomized, double-blind clinical trial comparing cefepime plus metronidazole with imipenem-cilastatin in the treatment of complicated intra-abdominal infections. Cefepime Intra-abdominal Infection Study Group. Arch Surg, 1997. 132(12): p. 1294-302. 9. Flake, A.W., Necrotizing enterocolitis in preterm infants--is laparotomy necessary? N Engl J Med, 2006. 354(21): p. 2275-6. 10. Moore, T.C., Successful use of the "patch, drain, and wait" laparotomy approach to perforated necrotizing enterocolitis: is hypoxia-triggered "good angiogenesis" involved? Pediatr Surg Int, 2000. 16(5-6): p. 356-63. 11. Schwartz, M.Z., et al., Intestinal stenosis following successful medical management of necrotizing enterocolitis. J Pediatr Surg, 1980. 15(6): p. 890-9. |
Pediatric EM Blog
AuthorPediatric EM Fellows at CMC/Levine Children's Hospital. Archives
November 2016
Categories
All
Disclaimer: All images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
